B e f o r e :
HIS HONOUR JUDGE HACON
(SITTING AS A HIGH COURT JUDGE)
____________________
Between:
| |
EDWARDS LIFESCIENCES LLC
|
Claimant
|
| |
- and -
|
|
| |
BOSTON SCIENTIFIC SCIMED, INC.
- and -
(1) EDWARDS LIFESCIENCES CORPORATION
(2) EDWARDS LIFESCIENCES AG
(also known as EDWARDS LIFESCIENCES SA)
(3) EDWARDS LIFESCIENCES LIMITED
|
Defendant
Third Party
Fourth Party
Seventh Party
|
____________________
Piers Acland QC and Miles Copeland (instructed by Powell Gilbert LLP) for the Claimant and the Third, Fourth and Seventh Parties
Richard Meade QC and Kathryn Pickard (instructed by Olswang LLP) for the Defendant
Hearing dates: 18-20, 23-24 and 26-27 January 2017
____________________
HTML VERSION OF JUDGMENT APPROVED�
____________________
Crown Copyright ©
Judge Hacon :
Introduction
- The defendant ("Boston") is the proprietor of two European patents, both of which claim inventions entitled "Repositionable heart valve". A valve of the type in issue is introduced percutaneously, i.e. using a needle-puncture of the skin to introduce a catheter into a blood vessel, via which the valve is pushed into position. This is to be contrasted with procedures involving the installation of valves by open heart surgery. The valves in the present case were often referred to as 'transcatheter heart valves' or THVs.
- The claimant sought revocation of Boston's EP (UK) 2 749 254 ("254") and EP (UK) 2 926 766 ("766") patents ("the Patents"). They are both divisional patents derived from the same parent application. The relevant priority date for both was 23 December 2003. The description in the specification of each of the Patents is largely the same.
- Boston counterclaimed for infringement and brought additional claims against five other companies in the same group as the claimant. The Fifth Party was in fact the same as the Fourth Party (being Swiss, it alternatively uses German or French designations) and the claim against the Sixth Party was later dropped. That left the claimant and three remaining companies as defendants in the additional claim, all of them part of the same group. I need not distinguish them and will refer to them individually and collectively as 'Edwards'.
- Despite this being formally a claim for revocation with a counterclaim for infringement, the trial went forward in the usual way, as if Boston were the claimant in an infringement action against Edwards. The product alleged to infringe is Edwards' Sapien 3 THV.
- Edwards argued that both the 254 and 766 Patents lacked novelty and inventive step, relying on four items of prior art. A squeeze was run against both Patents, alleging in each case that if the invention claimed was not obvious, necessarily it was not sufficiently disclosed in the specification. Finally, there was an allegation of added matter in relation to both.
- In argument attention was paid only to claim 1 of each Patent, save for a brief reference to other claims in the context of infringement of 254. Subject to that, I need therefore consider only the first claims of the Patents.
- Richard Meade QC and Kathryn Pickard appeared for Boston, Piers Acland QC and Miles Copeland for Edwards.
The technical background to the inventions
- The parties provided me with a helpful primer, largely plagiarised from the judgments of Kitchin J in Edwards Lifesciences AG v Cook Biotech Incorporated [2009] EWHC 1304 (Pat) and of Mr Peter Prescott QC in Corevalve Inc v Edwards Lifesciences AG [2009] EWHC 6 (Pat). It was common ground that everything in the primer formed part of the skilled person's common general knowledge as does, therefore, the following shortened form.
The Aortic Valve
- The cardiovascular system is divided into the pulmonary circulation which supplies blood to the lungs and the systemic circulation which supplies blood to the rest of the body. The two circulations are each maintained by the rhythmic contractions of the heart, in the case of the pulmonary circulation by the right ventricle and in the case of the systemic circulation by the left ventricle.
- The end of the pulmonary circulation is marked by oxygenated blood returning from the lungs to the heart via the pulmonary vein, entering the left atrium. From there it passes to the left ventricle, ready to be pumped around the rest of the body the systemic circulation. Between the left atrium and the left ventricle there is a valve: the mitral valve. When the left ventricle contracts, the mitral valve closes preventing the blood from flowing back into the left atrium. Instead the blood flows under high pressure into the main artery of the systemic circulation, the aorta.
- The phase in which the ventricle contracts is known as 'systole', as opposed to the phase in which the wall muscle relaxes and the ventricle expands, which is known as 'diastole'.
- Between the left ventricle and the aorta is the aortic valve. As diastole begins pressure inside the ventricle rapidly drops, falling below that of the blood in the aorta. The difference in pressure causes the aortic valve to close so that the blood does not return to the left ventricle during its expansion in preparation for a further contraction.
- The following is a diagrammatic representation of the location of the aortic valve between the left ventricle and the aorta.
.png)
- In this diagram the aortic valve is represented by two leaflets. In about 1-2% of the population, mostly males, there are indeed two leaflets, but in the rest of the population there are three. These leaflets are flaps of tissue which operate as the valve. When the left ventricle contracts, the pressure of blood pushes the leaflets apart, allowing the blood through. When the contraction ends at the start of diastole, the difference in blood pressure across the aortic valve is around 120 mm Hg. The consequent push of blood back towards the ventricle causes the leaflets to fall together, blocking the flow.
- It will be seen that the aortic valve sits in the aortic valve annulus, a narrowing that marks the division between aorta and ventricle. Also shown in the diagram are the coronary ostia, within a few millimetres of the leaflets. These are openings within the aortic sinuses. They lead to the coronary arteries which supply blood to the muscle of the heart wall and have some significance here because it is essential that these are not blocked when a THV is installed.
- The aorta in the diagram above is marked 'ascending aorta'. It is connected via an arch to the descending aorta. These are shown in the diagram below along with the coronary arteries and other arteries which branch off the aorta and form part of the systemic circulation. A THV intended to replace the aortic valve is usually passed up the descending aorta, via the arch, down into the ascending aorta and thence to the native valve.
.png)
Heart Valve Disease
- Heart valve disease may be congenital or it may be acquired. If acquired, it is often the aortic or mitral valve that will be affected. The most common afflictions are stenosis and regurgitation. In the former condition the leaflets of the valve fail to open fully, blocking the passage of the blood into the aorta or left ventricle as the case may be. If the patient suffers from regurgitation, the leaflets do not fall together to form a tight seal. Consequently some blood leaks backwards.
- These are not mutually exclusive conditions. Both are commonly caused by degenerative calcification, which is the accumulation of calcium carbonate in the leaflets and the parts of the heart surrounding the valve. The calcium carbonate collects to form very hard nodules, stiffening the tissue in which they form.
Replacing Defective Heart Valves by Surgery
- Surgeons have been replacing defective heart valves in patients for about 40 years. The only way of doing this until shortly before the priority date was by open heart surgery, taking 3-4 hours. The patient's chest is opened, the defective valve is cut out and an artificial valve is sewn into place. A general anaesthetic is required, as is the use of a heart-lung machine. This is still a commonly performed method of replacing heart valves but it is traumatic and is not suitable for fragile patients, who are liable to be killed by the procedure.
- The replacement valves used in open heart surgery take various forms. Some are mechanical. These have a long life span but tend to cause thrombus formation (blood clots) which require the patient to undergo life-long anti-coagulation therapy. Others are biologically derived. The leaflets are either homograft (human whole valves), xenograft (animal whole valves) or fabricated (tailored from animal pericardium, the tissue that covers the outside of the heart). In each case they are mounted within a textile cuff, or in a metallic or plastic frame.
Interventional Cardiology
- In the 1960s a new branch of medicine emerged known as 'interventional cardiology', that is to say the practice of treating patients with heart problems percutaneously rather than by surgery. It was and remains the province of physicians rather than surgeons. Physicians specialising in this field have become known as 'interventional cardiologists'.
- In 1977 the first human balloon angioplasty procedure was performed. A catheter carrying a balloon was inserted into an occluded human coronary artery and then expanded to force the artery open. In the 1980s other procedures were developed, including valvuloplasty: inflating a balloon catheter to open up a stenotic heart valve.
Stents
- During the 1980s and 90s there was a related development, namely the design of expandable stents to treat occluded vessels, in particular coronary arteries. These stents have an initial structure of narrow diameter to permit percutaneous introduction in a catheter. Then, once in place, they are expanded in diameter to form a scaffold inside the artery to hold it open. By the year 2000 stents were preferred over balloon angioplasty because they were less likely to result in restenosis (re-occlusion).
- Stents essentially fall into two categories. The first are those which are balloon expandable. Once the stent has reached its destination, a balloon inside is expanded to force the stent open by plastic deformation. The balloon is then deflated and the catheter withdrawn. The second category is self-expanding stents. These are made of a spring or 'memory metal', typically nitinol. They require a sheath to maintain the stent in its compressed form of narrow diameter. Once the stent is in place the sheath is withdrawn and the stent expands.
- Depending on the artery and condition to be treated, stents of differing diameters and lengths are required, and they are accordingly made in different sizes. By 2000 it was the general practice to size the stent to a diameter approximately 10-20% greater than the diameter of the vessel to be treated so as to ensure that it would exert radial pressure on the walls of the vessel and remain in place. It would also leave the lumen (the cavity of the vessel) unobstructed. Self-evidently, the narrower the diameter of the stent in compressed form, the greater is the range of vessels in which it can be introduced.
Transcatheter Heart Valves
- In the late 1980s THVs were developed, so avoiding the need for surgery, although at this time they were installed only in animals. In 1989 Dr Henning Andersen and his colleagues at Aarhus University in Jutland made a THV having an expandable metal frame, within which was a biological valve. This was implanted in pigs.
- In April 2002 Dr Alain Cribier and his team in Rouen performed the first implantation into a human being of a THV. It was installed in place of a native aortic valve. Dr Cribier's THV consisted of three bovine pericardial leaflets mounted within a balloon-expandable metal frame. By the priority date in December 2003 Dr Cribier had acquired celebrity status in his field for this breakthrough. Below are two images of Dr Cribier's valve, taken from a paper published in October 2003:
.png)
.png)
Transcatheter Access Routes
- Most interventional cardiology is performed using a needle inserted into the femoral artery (in the groin), although the radial artery (in the forearm) is sometimes used. The catheter is passed in a direction against the arterial flow of blood, thus known as the retrograde approach, towards the heart.
- There are other means, introducing the catheter by a needle into alternative arteries, including the aorta itself.
- Access to the heart can also be achieved using the antegrade approach, moving the catheter in the same direction as the blood flow. In this case the catheter is introduced into a peripheral vein, reaching the right side of the heart via the vena cava. If access to the left side is required, the catheter must be fed through the wall (known as the septum) between the right and left atria of the heart. This technique is used in particular to perform mitral valvuloplasty.
- The technique of replacing an aortic heart valve percutaneously has become known as 'transcatheter aortic valve implantation' or TAVI. It has made a dramatic improvement to the lives of many patients.
Terminology
- Strictly, the valve consists of the leaflets and is distinct from the frame. In many of the documents I was shown, the term 'valve' was used more loosely to mean the entire device. I will often do likewise. The exception is where I discuss the Patents because one of the arguments on the construction of the 254 Patent required the distinction to be maintained.
The inventions in summary
- The claimed inventions can best be described by reference to Dr Cribier's prior art device, shown above. (The precise form taken by the frame and leaflets of Dr Cribier's device are only illustrative in the context of summarising the inventions.) In both inventions a fabric skirt is provided on the outer lower part of the frame, thus encircling it. The device sits in the aortic valve annulus, pushing aside the diseased leaflets. The fabric skirt lies between the frame and the annulus or the frame and the native leaflets. It provides a seal, blocking the passage of blood that might otherwise pass around the outside the valve, between the frame and the annulus (or native leaflets). In other words, it prevents or limits what is known as paravalvular leakage, or PVL.
- The form taken by the fabric skirt is described in two ways in the specifications. The first form is claimed in 254: the seal is 'bunched up' in the deployed configuration. The second is claimed in 766: the seal takes the form of 'at least one sac'. Boston's case was that the seal could take either or both forms, whereas Edwards argued that they are mutually exclusive, a dispute I will come back to.
The Person Skilled in the Art
- It was common ground that the skilled team comprised a clinician and a bio-medical engineer. Boston submitted that the clinician was either an interventional cardiologist or alternatively a cardiac surgeon, in the latter case provided that he or she had sufficient interest in TAVI. Edwards argued that the team would never include a cardiac surgeon; the clinician would necessarily be an interventional cardiologist.
- This potentially mattered because a cardiac surgeon would bring with him or her (hereafter the possibility of either is to be inferred) common general knowledge that would otherwise be absent.
- The classic characterisation of the person skilled in the art was provided by Lord Diplock in Catnic Components Ltd v Hill & Smith Ltd [1982] R.P.C. 183. He identified the addressees of a patent specification thus (at p.242):
"those likely to have a practical interest in the subject matter of [the] invention (i.e. 'skilled in the art')"
Lord Diplock went on to add to this description (at p.243):
"persons with practical knowledge and experience of the kind of work in which the invention was intended to be used"
- So however well read-up an individual may be in a particular art, he will not qualify as a skilled person unless he has practical knowledge and experience in the relevant field. Practical knowledge and experience will bring in train common general knowledge that the 'library' expert in the field will not possess.
- To include a cardiac surgeon in the skilled team, I had to be satisfied that at the priority date such individuals possessed practical knowledge and experience in TAVI. Professor Georg Lutter was Boston's expert clinician. He said that in late 2003 it was extremely unusual for a heart surgeon even to be interested in TAVI. Most had significant reservations for several apparently good reasons and in particular because TAVI did not involve removal of the diseased valve, as would be done in a surgical replacement. Professor Lutter was one of the rare exceptions in that he was interested in TAVI but he had no practical experience and even he, at the time, seemed to be primarily interested in a TAVI procedure that could include ablation (i.e. excision) of the diseased valve at least in part. Only a small number of groups were working on TAVI devices in late 2003. Professor Lutter did not suggest that any of them included a cardiac surgeon.
- This does not necessarily exclude the cardiac surgeon from playing a part in the knowledge to be ascribed to the skilled team. In Pfizer Ltd's Patent [2001] FSR 16, Laddie J accepted (at [67]) that if an item of prior art flags a technology in which the skilled team are inadequately skilled, they would consider getting help from someone else. This raises the question whether the interventional cardiologist and the bio-medical engineer in the present case, exploring a very new field, should be assumed to have taken advice from a cardiac surgeon with practical experience in replacing heart valves. On the evidence before me, if the skilled team had consulted a cardiac surgeon in December 2003 and were lucky enough to find one with a positive attitude towards TAVI, they would have been advised to use a procedure in which the diseased leaflets were at least partially ablated. With hindsight it can be seen that the contribution from the notional cardiac surgeon would have been negative.
- In my view the skilled team consisted solely of an interventional cardiologist and a bio-medical engineer.
The Witnesses
- I have already mentioned Boston's clinical expert witness, Professor Georg Lutter. He is Professor of Cardiac Surgery at the University of Kiel and Head of the Department of Experimental Cardiac Surgery and the Heart Valve Replacement Department. Despite being a surgeon, Professor Lutter has carried out many TAVI procedures at Kiel. For most of these procedures Professor Lutter used Edwards' Sapien 3 device, having implanted about 250 of these by the time of giving evidence.
- My impression was that Professor Lutter was generally a good witness despite occasionally displaying what seemed to me to be a rather drawn out reluctance to accept matters of practice known at the priority date, matters made evident by contemporaneous documents.
- Boston's other expert was Professor James Moore. He is currently Professor of Biomedical engineering at Imperial College London. Professor Moore's particular expertise is in the field of stents.
- Professor Moore has given expert testimony in nine patent infringement cases in the United States, in five of which he was an expert on behalf of Boston. I mention this because, I regret to say, in the course of listening to Professor Moore I formed the impression that he has also developed what he might regard as an expertise in giving evidence. Professor Moore was extremely careful in giving his answers. I increasingly took the view that this was because his first priority was to avoid saying anything that might damage Boston's case. Assisting the court with his honest views was only a secondary motivation, at best. This was not helpful. I do not suggest that Professor Moore was going out of his way to mislead the court. But if a witness prevaricates at length over any answer that might not help the position of his side, the court is unlikely to accord much weight to his evidence as a whole. There will always be a strong suspicion of persistent bias.
- This must be put into perspective. Rarely, if ever, is an expert witness wholly objective by the time of the trial. Such is the effect of being part of a litigation team for which the focussed goal is, understandably, winning the argument. And, after all, there is a selection process. Nevertheless many experts find it possible to make appropriate concessions where their honest views require agreement with a point being put by counsel. No expert may be entirely objective but many are willing at least to give priority to assisting the court with accurate and helpful technical evidence.
- This takes me to Edwards' experts. Their expert clinician was Dr Nigel Buller. Dr Buller is a retired consultant cardiologist. Until 2008 he was Head of Interventional Cardiology at the Queen Elizabeth Hospital, Birmingham and the lead clinician for its cardiac catheterisation laboratories. During the course of his career Dr Buller developed an interest in interventional cardiology and had hands-on experience with the insertion of coronary stents. TAVI procedures were not used in the UK until 2008, a while after the priority date, by which time Dr Buller had stopped performing invasive procedures. He later received some training in TAVI at the New York Presbyterian Hospital in 2013.
- Dr Buller, like Professor Moore, has experience of being an expert witness in several proceedings, both in this country and in the United States. There the comparison ends. I found Dr Buller to be an excellent witness. He gave clear and direct answers without undue delay whenever he was able to. My impression was that Dr Buller was occasionally susceptible to hindsight and liable to accord more creativity to the skilled person than was appropriate in law. This, though, is not a criticism, just an observation.
- Edwards' expert on biomechanical engineering was Professor John Fisher. He has been Professor of Mechanical Engineering at the University of Leeds since 1993 and is current Pro-Vice-Chancellor for Research at that university. He is also a director of four externally funded centres of research into medical engineering.
- Professor Fisher did not claim any in-depth knowledge of TAVI procedures although he had read some of the commercial and academic literature in that field. He was a good witness so far as his evidence went.
Common General Knowledge
The law
- There was no dispute about the law. The general principles are well established and this was not a case which turned on a particular aspect of the law regarding what falls within or outside the common general knowledge. Recently Kitchin LJ provided the following summary in Idenix Pharmaceuticals Inc v Gilead Sciences Inc [2016] EWCA Civ 1089:
"[72] It follows that the common general knowledge is all that knowledge which is generally regarded as a good basis for further action by the bulk of those who are engaged in a particular field. It is that knowledge which those working in that field will bring to bear when they are reading or learn of a piece of prior art. It is not necessary that those persons have that knowledge in their minds, however. The common general knowledge includes material that they know exists and which they would refer to as a matter of course if they cannot remember it and which they understand is generally regarded as sufficiently reliable to use as a foundation for further work."
This case
- The parties were agreed that the contents of the primer formed part of the common general knowledge including, in particular, the celebrated work done by Dr Cribier not long before the priority date. The first implantation of a THV into a patient's aorta was done by his team in April 2002. The patient was a man aged 57 who died 17 weeks later, although for reasons unrelated to the valve implantation. The work was presented in a paper delivered by Dr Cribier to a conference in Washington in September 2002 and was also published as a special report in the journal Circulation in December 2002 ("the 2002 Cribier paper").
- Dr Cribier was also one of the authors of a review paper published in 2003 in the British Journal of Cardiology ("Dalby"). Dalby reported that a further three patients had been treated using TAVI. The second died because the THV could not be properly implanted and was ejected into the aorta. In the third and fourth cases the implantation was successful.
- Professor Lutter referred to a review paper of which he was the leading author, published in Annals of Thoracic Surgery in December 2004, reviewing literature no later than May 2004. Professor Lutter said that given the delay of scientific publications, this provided a reasonably contemporaneous record of the state of TAVI in December 2003. This was not challenged. The paper included the following (omitting footnotes):
"A number of technical difficulties were encountered in the early phases of percutaneous valve replacement, which to varying degrees still exists. These difficulties include optimal attachment of the valve into the stent, preservation of the function of the valve stent after compression and re-expansion, a suitable visualization method, functional anchoring mechanism, and avoidance of paravalvular regurgitation and obstruction of coronary orifices in aortic implantation."
- Thus, avoiding or at least minimising PVL was one of the concerns of those interested in TAVI. Boston identified three areas of dispute with regard to the common general knowledge of the skilled person in December 2003, although this expanded during argument:
(i) The extent to which PVL was known to be a problem in TAVI procedures and the precise nature of likely PVL.
(ii) The extent to which surgical replacement valves were known, i.e. the type of valves sewn into patients during open-heart surgery.
(iii) The extent to which stents or endografts were known.
- An endograft is a stent with an external fabric covering. It is introduced into an artery and deployed at the site of an aneurysm, then expanded. Blood flows through the channel within the endograft thereby relieving the pressure on the aneurysm in the artery wall.
Knowledge of the types of PVL
- For the purpose of his evidence at trial, Professor Lutter divided leakage in the context of an aortic valve into three types. Type 1 leakage occurs when blood passes through defective leaflets, i.e. through the valve itself. This is the leakage which results in regurgitation in diseased native valves but can also occur in defective replacement valves.
- Leakage of Types 2 and 3 occur only with replacement valves. Type 2 happens when the valve is not accurately placed in the annulus, so that the leaflet in the replacement valve does not meet the frame at the point where the frame is in contact with the annulus. Type 3 leakage could happen whether the valve was accurately positioned or not. It is leakage between the annulus and the frame. The distinction is best demonstrated using Professor Lutter's diagrams: below are two forms of Type 2 leakage and then Type 3:
.png) Type 2 leakage
Type 2 leakage
.jpg) Type 3 leakage
Type 3 leakage
- In his report Professor Lutter suggested that Type 3 leakage was little known or understood in late 2003 and that to the extent that it was acknowledged, the skilled person would have expected to solve it by ablating the native leaflets. In the TAVI procedure, the native leaflets, generally studded with calcium nodules, are left in place, squashed against the annulus. In December 2003 there was no practised method of ablating the leaflets.
- I think the picture presented by Professor Lutter was contradicted by papers published at around the priority date. These included a paper about the new TAVI procedure published in April 2002 in The Journal of Thoracic and Cardiovascular Surgery, with Professor Lutter as lead author ("the 2002 Lutter paper"). At this time Professor Lutter and his colleagues practised TAVI in pigs. At the end of the article there are comments from Dr Alain Carpentier, a renowned cardiac surgeon:
"We also know from clinical practice, that if you leave even a small peripheral leak, it has some very often important deleterious effect, even a rather small leak, either haemolysis or insufficiency. Knowing that you will never be able to remove all the calcium formation, then you have a high risk of having peripheral leak. How can you solve that problem?"
- While it is not certain what Dr Carpentier had in mind, 'peripheral' leakage sounds very much like Type 3. Dr Carpentier's view, a year and a half before the priority date, was that the presence of calcium nodules in the native leaflets and artery wall and the difficulty of removing them created a high risk of 'peripheral' leakage, a problem to which there was no obvious solution.
- Dr Buller was cross-examined on this topic. He said that he could not disagree more with Professor Lutter: that at the priority date those in the field did not distinguish between Professor Lutter's Type 2 and Type 3 leakage. PVL was known and just thought of as blood flowing round the outside of the valve, as opposed to through the valve. I accept that evidence. There was no sign that anyone had considered Type 2 leakage in advance of Professor Lutter's report for this trial. Even Professor Lutter in cross-examination conceded that in 2003 no distinction was drawn between Type 2 and Type 3 leakage in relation to the mild regurgitation reported following Dr Cribier's TAVI procedures.
- In my view the skilled person at the priority date would have contemplated leakage and would have mainly considered the possibility of blood leaking around the outside of any implanted valve. Hereafter my references to 'PVL' are to be given that meaning, i.e. Professor Lutter's Type 3.
- A separate although related argument was advanced by Boston, particularly in closing: at the priority date PVL was not considered to be a big problem. Paravalvular regurgitation was described as 'moderate' in the 2002 Cribier paper and Dalby referred to Dr Cribier's work as having resulted in 'only a small paravalvular leak'.
- In May 2012 Dr Susheel Kodali and other authors published what Dr Buller described as an important paper in the New England Journal of Medicine: Two-Year Outcomes after Transcatheter or Surgical Aortic-Valve Replacement. It reported that the rates of death in patients in the two years following TAVI or surgical valve replacement were in both cases about 35%. Among other things, the authors stated
"aortic regurgitation (even mild) after TAVI was associated with increased long-term mortality."
A follow-up review of the literature was published in March 2013 in the Journal of the American College of Cardiology entitled Paravalvular Leak After Transcatheter Aortic Valve Replacement, The New Achilles' Heel? The lead author was Dr Philippe Généreux. It included this:
"More disturbingly, although it was generally believed that only moderate or severe regurgitation would impact long-term outcomes, the recently published 2-year results from the PARTNER trial showed that even mild PVL was associated with significant mortality
[footnote reference to the Kodali paper]"
- Dr Buller described the 2012 finding that mild PVL was associated with significant mortality as having been disturbing and not one that had been expected. Dr Carpentier, a surgeon, seems to have taken PVL more seriously than most (see the 2002 Lutter paper) but his appears to have been a minority view and possibly one influenced by his experience as a surgeon.
- I find that in December 2003 PVL would have been perceived by the skilled person as a problem, to be eliminated if at all possible, but not one that was likely to be a significant cause of mortality following TAVI.
- The evidence showed that the principle means for tackling PVL in the context of TAVI was by ensuring that the stent, once installed, applied a strong radial pressure against the annulus. This could be achieved by oversizing the stent or using a balloon to re-expand the stent if PVL was observed.
Knowledge of surgical replacement procedures
- Dr Buller and Professor Lutter differed as to the common general knowledge of the interventional cardiologist with regard to surgical replacement valves.
- The limited relevance of this aspect of the evidence was that a knowledge of surgeons' practice of tightly suturing a valve into place by a surgeon would imply knowledge that PVL can occur and should be reduced as much as possible. It might also have encouraged the idea that the site should be cleared of calcium to improve the likelihood of a close fit between valve and annulus.
- For reasons discussed above, I think that the skilled team would have been fully aware of the possibility of PVL and the desirability of minimising it following the replacement of a valve surgically or by TAVI. Their views on this in the context of TAVI would have been guided by reports of the work done by Dr Cribier rather than the surgical replacement of valves.
Endografts
- One of the cited items of prior art was an endograft on which Edwards based an argument on obviousness. Attention was also paid to endografts more generally as a source of common general knowledge which, according to Edwards, would have been applied in the context of TAVI at the priority date.
- The skilled team would have known of endografts, their purpose and how they worked in general terms. It was common ground that this would include the need for a tight seal with the artery wall at either end of the endograft to ensure that blood did not flow into the aneurysm and risk its bursting.
The Gore Excluder
- In his report Dr Buller said that in the period before the priority date all commercialised stents with non-elastic covers had coverings of greater diameter than that of the intended deployed stent so that the expansion of the stent in use would not be constrained. The presence of excess fabric led to wrinkles in it and paths along which leaks could occur. To deal with this W.L. Gore & Associates Ltd manufactured an endograft with a Gore-Tex covering ("the Gore Excluder"), featuring a cuff at each end which flared out and, according to Dr Buller, was intended to operate as an additional seal against blood flow. Dr Buller said the Gore Excluder was well-known at the priority date.
- Dr Buller exhibited Gore's instructions for using a Gore Excluder. It illustrated the cuff, referring to it as a 'sealing cuff'. But it was neither shown nor described as being flared and there was nothing in the instructions or elsewhere in the documents presented at trial to indicate how it worked.
- The Gore Excluder was one of about a dozen devices used for endovascular repair of abdominal aortic aneurysm ("AAA") at the priority date. Only the Gore Excluder had a cuff. Dr Buller said that he never used the Gore Excluder himself, but he was familiar with it from the literature. It turned out that Dr Buller's view of how the sealing cuff on the Gore Excluder worked had been prompted by reading one of the cited items of prior art, referred to as 'Thornton'.
- It seems that in the course of these proceedings Dr Buller read Thornton and then looked at the cuff on the Gore Excluder with new eyes. I think this was an example of Dr Buller's thinking that could be more imaginative than that of the skilled team.
- I am not satisfied that the evidence established how the cuff on the Gore Excluder actually worked and in particular whether it flared out and thereby provided a seal against blood flow. I do not believe that Dr Buller's current view on how it worked reflects the common general knowledge of the skilled person at the priority date.
- Thornton is the cited prior art, not the Gore Excluder. It must be taken on its own merits, so I need say nothing further about the Gore Excluder.
The location of endografts
- Edwards argued that the skilled team would have perceived parallels between the seals used in endografts and those required for a replacement valve used in a TAVI procedure.
- It was established that those using endografts in December 2003 aimed to implant them at sites of healthy tissue and indeed the instructions for use discouraged implantation at sites where calcification was present. In some circumstances, however, it may have been necessary for endografts to be attached at sites in calcified, irregular vessels. Calcification could cause difficulties in delivery of the device to the required site. It was not shown that, as part of their common general knowledge, the skilled team would have perceived calcification at the point of fixation to be a cause of leakage and thus a problem to be addressed when using endografts.
Foreshortening
- When a THV is located at the site of implantation, its diameter is expanded to fix it there permanently. Sometimes the construction of the frame is such that as its diameter expands, its length shortens. This is known as 'foreshortening'. Dr Buller and Professor Moore agreed that at the priority date it was part of the skilled team's common general knowledge that in most situations it would be better to use a stent that foreshortened only a little or not at all and that THVs could be made with a frame that did not foreshorten.
Desirable characteristics of a THV
- In cross-examination Dr Buller accepted that at the priority date the skilled team, as part of their common general knowledge, would have had in mind a number of features which they would have regarded as being either essential or desirable in a THV. These were as follows, although I have run some of them together where they are closely connected:
(1) It had to work as valve and so it had to allow blood to flow sufficiently during systole and provide a seal and resist leakage during diastole.
(2) It had to be possible to anchor the THV firmly to the vessel once on site; thus the frame had to exert the necessary radial force.
(3) It had to last.
(4) It had to be possible to deliver the THV by catheter to the required site and thus it had to have a low delivery profile and a functional delivery system.
(5) It had to be possible to position the THV accurately; among other things this might affect the degree of foreshortening desirable.
(6) It had to be visible to the physician using imaging systems available.
(7) It had to be of a shape which did not interfere with other parts of the anatomy, e.g. by occluding coronary arteries.
(8) It had to incorporate an appropriate means of expansion, i.e. balloon or self-expansion.
(9) Manufacturing costs had to be minimised to the extent possible.
(10) It had to be compatible with any necessary medical considerations, such as an anti-coagulant regime undertaken by the patient.
- I don't believe that any of these were in dispute. At the priority date the skilled team would have known that all these desirable criteria could be satisfied: Dr Cribier and his team had done so. Boston's point, as I understood it, was that at the priority date, part of the common general knowledge of the skilled team contemplating making a better THV would have been that any of the above criteria were candidates for improvement and that all had still to be sufficiently met. I accept that.
The Patents
- The invention claimed in both Patents is a THV with a fabric skirt around the exterior of the 'anchor', the name given in the patents for the frame. The skirt acts as, and is called a 'seal'.
The 254 Patent
- The key part of the invention is that in the deployed configuration of the device, the skirt of the THV is 'bunched up'.
- Claim 1, divided into integers, is:
(i) Apparatus for endovascularly replacing a patient's heart valve, the apparatus comprising:
(ii) an expandable anchor
(iii) supporting a replacement valve,
(iv) the anchor having a delivery configuration and a deployed configuration,
characterized by
(v) a fabric seal
(vi) extending from the distal end of the valve
(vii) proximally over the anchor in the delivery configuration
(viii) wherein the seal is bunched up in the deployed configuration.
- To create a seal around the valve the skirt must be deployed between the valve and the wall of the artery. In preferred embodiments, claimed in claim 13, at least a portion of the seal is adapted to be captured between the native leaflets and the heart wall.
- Claim 1 does not require foreshortening (this is claimed in claim 9). Claims 2 and 3 suggest that the creation of flaps and pockets in the fabric (claimed in claim 2) is distinct from the creation of pleats (claimed in claim 3).
The 766 Patent
- In the invention claimed in the 766 Patent the seal is created by at least one sac disposed around the exterior of the anchor (i.e. frame) of the THV. The sac or sacs may be filled with water, blood, foam, a hydrogel or other materials. Slots or pores may be present in the sacs to allow them to fill with blood passing through the valve.
- Claim 1 reads:
(i) Apparatus for endovascularly replacing a patient's heart valve, the apparatus comprising:
(ii) an expandable cylindrical anchor
(iii) supporting a replacement valve,
(iv) the anchor having a delivery configuration and a deployed configuration,
(v) and at least one sac disposed about the exterior of the anchor to provide a seal.
- Like claim 1 of 254, claim 1 of 766 does not require foreshortening (see claim 13).
Construction
The law
- The general principles of law on the construction of patent claims are well established, see Kirin Amgen Inc v Hoechst Marion Roussel Ltd [2004] UKHL 46, [2005] RPC 9 at [18]-[52] and Virgin Atlantic Airways Ltd v Premium Aircraft Interiors UK Ltd [2009] EWCA Civ 1062, [2010] RPC 8 at [5]. The court must identify what the person skilled in the art would have understood the patentee to be using the language of the claim to mean.
- Edwards advanced a particular point which arose out of what the Court of Appeal said in Virgin. In that case, as in this, the parent application described more than one invention. In Virgin one of the inventions was a herringbone arrangement of business class seats in a plane, called 'the space-packing idea'; a second was a business class seat which was flipped over when converted into a bed. A number of divisional applications emerged, one of which matured into the patent in suit. This contained claims confined to the space-packing idea. However the description in the patent only disclosed an embodiment of that idea which was also a flip-over seat. At first instance the judge held that the claims were therefore limited to the space packing idea as used in flip-over seats. The Court of Appeal disagreed. Jacob LJ, giving the judgment of the Court, said:
"[15] We think it would unrealistic indeed perverse for the law to say that the notional skilled reader, probably with the benefit of skilled advice, would not know and take into account the explicit drafting conventions by which the patent and its claims were framed. Likewise when there is a reference to the patent being a divisional application, it would be perverse to work on the basis that the skilled man would not know what that means. A real skilled man reading a patent which, as in the case of the Patent, refers to 'the parent application' would surely say 'what's a parent application?' and he would go on to ask a man who knows, probably a patent agent."
- Informed by knowledge of divisional applications, the skilled person would construe the claims to the space-packing idea accordingly:
"[48] The 'lost space' and the space-packing idea of using the bed to extend into it is self-evidently wholly unrelated to whether the bed flips over or not. So the skilled reader would have no reason to suppose that the patentee intended to limit his claim to flip-over bed/seats.
[49] Now it is of course true that the only specific embodiment is a flip-over bed/seat. And, because that would strike the notional skilled reader as a good idea he would expect it to be patented somewhere. But because he knows (see above) that the patentee has divided out what is in this patent from a parent application he would not necessarily expect that to be done in this patent.
[54] So we think the notional skilled reader would go by the claim and not look for or expect any hidden limitations in it."
- Knowledge of divisional applications would open the skilled person to a possible explanation for an apparent inconsistency between the claims and the description. I do not believe that the Court of Appeal intended this to have the effect of putting rigid assumptions into the mind of the skilled person. Specifically, the skilled person would know that in any context inventions can overlap a single product or process might embody more than one invention. In the context of a patent derived from a divisional application, the skilled person would therefore not assume that an example of the claimed invention, as described or illustrated in the specification, embodies only that invention. It might, but equally it could also embody one or more of the other inventions claimed in the parent application. Subject to an indication in the specification one way or the other, the skilled person would contemplate any possibility.
The 254 Patent
- There were a number of issues on construction which I will take in turn.
A fabric seal
- The skilled person would understand from the description that sealing occurs in the deployed configuration of the apparatus and in this configuration the seal is "adapted to prevent blood flow around the replacement valve and the anchor when the anchor and the replacement valve are fully deployed" (col. 4, lines 17-19).
A [fabric seal] extending from the distal end of the valve proximally over the anchor in the delivery configuration
- In this context it is important to keep in mind the distinction between the frame, referred to as the 'anchor' in the Patent, and the valve, i.e. the replacement leaflets located within the frame.
- In the delivery configuration the seal extends from the distal end of the valve proximally over the anchor. It was common ground that in this context the 'distal' end is the end from which blood flows into the valve; the other is the 'promixal' end.
- Edwards referred to paragraph [0062]:
"[0062] Figures 22-24 show another way to seal the replacement valve against leakage. A fabric seal 380 extends from the distal end of valve 20 and back proximally over anchor 30 during delivery. When deployed, as shown in figures 23 and 24, fabric seal 380 bunches up to create fabric flaps and pockets that extend into spaces formed by the native valve leaflets 382, particularly when the pockets are filled with blood in response to backflow blood pressure. This arrangement creates a seal around the replacement valve."
- Figures 22-24 are shown below. In figures 22 and 23 the distal end is the lower end and the proximal end is uppermost. The valve is shown diagrammatically as a cylinder, but would in fact consist of the leaflets. These would be attached to the frame at the bottom, leaning against each other towards the top.
.png)
- Edwards argued first that the fabric seal must extend only in a proximal direction from the distal end of the valve, i.e. the point of attachment of the leaflets to the anchor. Any distal extension, including distal extension of the inner skirt, is ruled out. Their second point concerned the proximal extension of the fabric over the anchor, i.e. the outside of the frame. There must be extension from the distal end of the valve. Therefore, Edwards argued, there must be at least some fabric on the outside of the frame proximally beyond the level at which the leaflets are attached to the anchor on the inside higher up if one is looking at figure 22.
- I do not accept that the skilled addressee would understand the specification and the claims in this sort of finely honed detail. All that is said about this aspect of the invention is contained in the second sentence of paragraph [0062] (see above). The only other guide is figure 22.
- Figure 22 suggests that that the fabric could start on the inside of the anchor, extend at first distally on the inside, fold around the end of the anchor and thereafter, now on the outside, extend proximally from the distal end. Neither in the description nor in the words of the claim is there a prohibition of distal extension of the fabric seal; just that there must be proximal extension.
- The figures of the 254 Patent place the valve at the bottom of the anchor. So the distal ends of the valve and anchor are more or less level. With that arrangement, if there is proximal extension of the fabric on the outside of the frame, the fabric is bound to extend proximally beyond the level of distal end of the valve higher up in figure 22. If the valve is located higher up the anchor the fabric on the outside might not extend as high as the lower end of the valve. The question is whether the skilled team would have understood the specification to mean that the patentee intended to embrace such an alternative arrangement as part of his invention? In my view, yes. Firstly, none of the experts suggested that this would make any difference to the way the invention worked. I think this would also have been obvious to the skilled team. Secondly, I think the skilled addressee would take the view that if such a precise connection between the positioning of the fabric on the outside of the frame and the point of attachment of the leaflets on the inside of the frame had been intended, it would have been much more clearly signalled.
The seal is bunched up in the deployed configuration
- 'Bunched up' is not a term of art. So Edwards began with a definition of the verb 'to bunch' taken from the Shorter OED: "Make into a bunch or bunches; gather (material) into close folds". This, I agree, provides a start although I would not place any great emphasis on 'close'. The term 'bunched up' must be given a purposive construction. The purpose of the bunched up fabric is to provide a seal in the deployed configuration. Thus, the fabric cannot be taut there must be excess fabric leading to the formation of folds when the device is used in the deployed configuration. There must be sufficient excess fabric such that it functions as a seal within the meaning referred to above.
- Edwards referred to figure 23 and while acknowledging that this is a diagrammatic representation of the bunching, argued that it accurately suggests horizontal folds since vertical ones would provide leakage paths for the blood. That makes sense to a degree, but I do not believe that the term 'bunched up' directly limits the direction or shape of the folds. If they were all vertical and as a consequence the fabric provided no seal, such an arrangement would not satisfy the claim because the functional requirement of a 'seal' would not be met.
- Thus, the seal is bunched up if it consists of sufficient fabric such that folds are created within it when the apparatus is deployed and also such that the fabric may move out against the vessel wall, conforming with its contours, and thus prevent blood flow around the apparatus to an extent which is at least significant.
Flaps, pockets and pleats
- In claim 2 the fabric bunches up to create flaps and pockets; in claim 3 to create pleats. Pleats are apparently distinct from flaps and pockets. Edwards again relied on the OED and it seems to me that pleats connote bunching in the form of a relatively regular series of folds.
The 766 Patent
At least one sac
- 'Sac' is a further term used in the patents which is not a term of art. Again, Edwards referred to the Shorter OED:
"sac noun
1 BIOLOGY. A natural baglike cavity in an organism; the membrane or other structure enclosing this.
2 MEDICINE. A pouch formed by the pathological dilation or protrusion of a part; the membranous envelope of a hernia, cyst, tumour, etc."
- The definitions suggest that acontextually the skilled team might think of a sac as either a cavity, or alternatively the membrane or other material enclosing the cavity, or both. Before resolving this I turn to the next point of construction.
Disposed about the exterior of the anchor
- There was a dispute about where the walls of a sac must be if, as claim 1 requires, the sac is disposed about the exterior of the anchor. Edwards argued that the words of the claim clearly indicate that the whole of the sacs, walls and all, must be on the exterior of the anchor. Edwards said that was consistent with paragraphs [0065]-[0067] of the specification and Figures 14-16. I will set the paragraphs out in full (omitting reference numerals) since they are the only paragraphs which deal directly with the sac invention:
"[0065] Referring to Figure 14, optional elements for reducing regurgitation or leakage are described. Compliant sacs may be disposed about the exterior of anchor to provide a more efficient seal along irregular interface I. Sacs may be filled with an appropriate material, for example, water, blood, foam or a hydrogel. Alternative fill materials will be apparent.
[0066] With reference to Figures 15, illustrative arrangements for sacs are provided. In Figure 15A, sacs are provided as discrete sacs at different positions along the height of anchor. In Figure 15B, the sacs are provided as continuous cylinders at various heights. In Figure 15C, a single sac is provided with a cylindrical shape that spans multiple heights. The sacs of Figure 15D are discrete, smaller and provided in larger quantities. Figure 15E provides a spiral sac. Alternative sac configurations will be apparent to those of skill in the art.
[0067] With reference to Figures 16, exemplary techniques for fabricating sacs are provided. In Figure 16A, sacs comprise 'fish-scale' slots that may be back-filled, for example, with ambient blood passing through replacement valve. In Figure 16B, the sacs comprise pores that may be used to fill the sacs. In Figure 16C, the sacs open to lumen of anchor and are filled by blood washing past the sacs as the blood moves through apparatus."
- Edwards had three further arguments. First, paragraph [0071] and Figures 27 and 28 (the same as figures 22 and 23 of the 254 Patent, shown above in paragraph 102) described an embodiment with part of the wall on the inside of the anchor, but this is in the context of a description of the invention clamed in the 254 Patent and so the skilled person would assume that these were not embodiments of the invention claimed in the 766 Patent. Secondly, paragraph [0019] of the specification referred to US patent application 2001/0039450 ("Pavcnik") as part of the prior art. Pavcnik discloses a valve with a sac having walls traversing the anchor. The skilled person would assume that the 766 Patent had not been framed to encompass the prior art and thus such embodiment of a sac. Thirdly, Dr Buller's evidence that if the inner wall of the sac were on the inner side of the anchor part of the inflation of the sac would be wasted. Edwards argued that the skilled person would not understand the 766 Patent to be claiming an embodiment that was sub-optimal in its function as a seal.
- Edwards' arguments are based on the premise that a 'sac' must consist of the walls or alternatively include both cavity and walls. If that is right and if the language of claim 1 were construed strictly, I agree this would lead to a conclusion that both walls of the cavity must be outside the anchor if that claim is to be satisfied.
- The reference in paragraph [0067] to sacs comprising slots or pores supports the inclusion of the walls as part of the sac and it seems to me that the skilled person would understand the sac to consist of the cavity and also its walls. Also, it is a sac and therefore must have ends which, at the minimum, are broadly perceptible. So the walls must at least approximately meet at each of the two ends.
- The skilled team must further be deemed to apply a purposive construction. The specification indicates the sacs are to be filled with appropriate material, such as ambient blood, and their purpose is to reduce regurgitation or leakage in that sense act as a seal. Dr Buller thought that if the inner wall of the sac was inside the anchor part of the inflation of the sac would be wasted. He did not say that such an arrangement would prevent the sac from reducing regurgitation or leakage. I have no reason to doubt that the sac could still function as a seal. It therefore seems to me that on a purposive construction of claim 1 the skilled team would believe that it does not matter whether the inner wall of the sac is inside or outside the anchor.
- I was not persuaded to a contrary view by Edwards' further three arguments. The first rests on an interpretation of what the Court of Appeal said in Virgin, an interpretation which I have rejected. The second is only good if Pavcnik would anticipate the invention claimed in the 766 Patent on Boston's construction of claim 1. Edwards did not suggest that it would and Professor Lutter's evidence indicated that it would not. The third I have already considered.
- A sac consists of a cavity created between the fabric of the inner and outer skirt, together with its fabric walls which at least approximately meet at its two ends. The inner fabric may be inside or outside the frame. The outer fabric must be adapted to move freely enough to lie sufficiently closely against the adjacent vessel wall, such as to reduce leakage to a significant extent.
Edwards' Sapien 3 Valve
- In 1999 Dr Cribier and others set up a company based in New Jersey, Percutaneous Valve Technologies ("PVT") to manufacture the valves he was to use in his work in Rouen in 2002. PVT was purchased by Edwards in 2004. Edwards marketed its first THV in 2005 under the trade name 'Sapien'. In 2009 this was replaced by the Sapien XT. Both the Sapien and Sapien XT had an inner skirt, that is to say fabric lining the inside of the frame. In 2014 Edwards launched the Sapien 3, the product alleged to infringe. It was the first to feature an outer skirt, which is sutured to the inner skirt and covers part of the outer surface of the frame. The outer skirt is designed to bulge outwards at its top end. Below is an image of the Sapien 3:
.png)
- It was common ground that Edwards designed the outer skirt to have the effect of minimizing PVL and marketed the Sapien 3 accordingly. It was also common ground that the skirt on the Sapien 3 successfully achieves that effect in use.
Infringement of the 254 Patent
- By the time of its closing submissions Edwards advanced three arguments of non-infringement. The first was that in the delivery configuration of the Sapien 3 the fabric seal does not extend proximally from the distal end of the valve. This was for two reasons: (a) the valve is not at the distal end of the device, so the inner skirt or seal must extend distally and (b) the outer skirt or seal does not extend proximally beyond the distal end of the valve. I have found above that both arrangements (a) and (b) fall within claim 1.
- Moreover, with regard to argument (b), Edwards' Product and Process Description ("PPD") indicated that the distal end of the valve, i.e. the point at which the leaflets are sutured to the inner skirt, undulates. Boston argued that figure 16 of the PPD showed that at some points the outer skirt extends proximally beyond the distal end of the valve. However, figure 16 showed the product in its deployed configuration. As against that, Edwards did not point to any disclosure in the PPD which established that in the delivery configuration the outer skirt of the Sapien 3 does not extend proximally beyond the line of suturing of the leaflets to the inner wall. There was one image, figure 18, which did not help. Edwards was under a duty to establish all relevant facts in its PPD. If not, an adverse inference is liable to be drawn, as I do here.
- Edwards' second argument was that the fabric seal in the Sapien 3 is vertically pleated in the delivery configuration but becomes smooth upon expansion of the device. Pleating in the delivery configuration is irrelevant to claim 1. The submission that the fabric seal becomes smooth upon expansion is a different way of putting Edwards' third argument.
- The third argument was that the fabric seal of the Sapien 3 is not bunched up in the deployed configuration. Before reaching any conclusion as to whether the fabric is bunched up, it was necessary to know how the fabric is shaped and behaves in use. Again, the PPD provided no clear information about this essential issue of fact. Boston complained about this before the trial and were provided by Edwards with a short video, which became known as the 'orange gasket video'. It provided an in vitro illustration of the effect of fluid flowing around the apparatus and what I took to be a reasonably accurate representation of what happens inside a patient once the Sapien 3 is deployed. The video showed part of the anchor. Radially outwards from the anchor was the outer skirt and then a gasket serving as the vessel wall. A notch had been cut into the gasket to simulate a gap through which blood would leak if the device were to be installed in vessel with an uneven wall. I was also provided with stills of the video.
- Mr Meade provided a commentary as the video was shown in court and suggested that the fabric could be seen to bulge out and to fill the gap, thereby sealing it, as fluid flowed around the apparatus. This is indeed what appeared to happen and Mr Acland did not dissent.
- I was also provided with a sample of the Sapien 3 and I have taken a close look at it.
- I have no real doubt that the outer skirt of the Sapien 3 has sufficient fabric such that folds would be created within it when the apparatus is deployed, whether because it is pressed against a vessel wall or, if not, because there is sufficient excess fabric for folds to occur in response to the flow of fluid around the apparatus. The skirt is bunched up within the meaning of claim 1.
- I have mentioned that the Sapien 3 is marketed on the basis that the outer skirt acts as a seal. It is enough for me to quote one example, taken from a press release issued by Edwards on 27 January 2014:
"The new [Sapien 3] valve has an outer skirt a cuff of fabric surrounding the valve frame providing a seal to address paravalvular leak. The effectiveness of this solution is supported by the limited clinical experience [reference to papers published in medical journals] as detailed in two first in-human feasibility studies, which demonstrated that significant paravalvular leak was eliminated during transcatheter aortic valve implantation (TAVI)"
- It follows from that indication from Edwards that the movement of the outer skirt against the vessel wall significantly reduces PVL.
- The Sapien 3 device falls within claim 1 of the 254 Patent. I also take the view that in its bunched up state the fabric seal will create flaps and pockets within it. Claim 2 is infringed. I think it unlikely that the folds will be sufficiently regular to qualify as pleats. Claim 3 is not infringed.
- Claim 6 requires the seal to bunch up in response to backflow blood pressure. The orange gasket video suggests to me that this is likely to occur. Claim 6 is infringed.
Infringement of the 766 Patent
- In closing Edwards argued that two elements of claim 1 of the 766 Patent were missing from the Sapien 3: there was no sac and there was only a single layer of fabric disposed outside the anchor.
- I have already found that the second of these is not a requirement of claim 1.
- As to the sac, for reasons already given I take the view that in the Sapien 3 there will be at least one ring-like cavity created between the fabric of the inner and outer skirt. Alternatively, in use the ring will be broken into smaller cavities. The outer skirt can move freely enough to lie sufficiently closely against the adjacent vessel wall such as to reduce leakage to a significant extent. Claim 1 is infringed.
- In closing neither Mr Meade nor Mr Acland pursued arguments in relation to further claims of the 766 Patent.
The Prior Art
- Four items of prior art were relied on in relation to allegations of lack of novelty and inventive step:
(1) International Patent Application, publication no. WO 98/29057 ("Cribier"). One of the two named inventors is Dr Cribier.
(2) US Patent No. 5,855,601 ("Bessler").
(3) US Patent No. 6,015,431 ("Thornton").
(4) International Patent Application, publication no. WO 02/36048 A1 ("Seguin").
Novelty
The Law
- There was no dispute about the law:
"In order to anticipate a patent, the prior art must disclose the claimed invention and (together with the common general knowledge) enable the ordinary skilled person to perform it: Synthon BV v Smithkline Beecham Plc [2006] RPC 10."
Per Lord Hoffmann, H. Lundbeck A/S v Generics (UK) Ltd [2008] EWCA Civ 311; [2008] RPC 19, at [9].
- I would add this. It is not essential that an item of prior art should expressly disclose all the features of an invention for that prior art to deprive the invention of novelty. It may be that one or more integers are disclosed by inference. But this must be an inevitable inference drawn by the skilled person reading the prior art. In Smithkline Beecham Plc's (Paroxetine Methanesulfonate) Patent [2005] UKHL 59; [2006] RPC 10, Lord Hoffmann, with whom the rest of the House of Lords agreed, considered the observations of Lord Westbury L.C. in Hill v Evans (1862) 31 L.J. Ch (NS) 457 at 463 and those of the Court of Appeal in General Tire and Rubber Co v Firestone Tyre and Rubber Co Ltd [1972] R.P.C. 457, at 485-486. On the facts of Smithkline Beecham Lord Hoffmann was concerned with the knowledge of the author of the prior art, but also emphasised that if the prior art allows even for the possibility that its performance would not result in the claimed invention, it will not deprive that invention of novelty:
"[22] If I may summarise the effect of these two well-known statements, the matter relied upon as prior art must disclose subject-matter which, if performed, would necessarily result in an infringement of the patent. That may be because the prior art discloses the same invention. In that case there will be no question that performance of the earlier invention would infringe and usually it will be apparent to someone who is aware of both the prior art and the patent that it will do so. But patent infringement does not require that one should be aware that one is infringing: "whether or not a person is working [an]
invention is an objective fact independent of what he knows or thinks about what he is doing": Merrell Dow Pharmaceuticals Inc v H N Norton & Co Ltd [1996] RPC 76, 90. It follows that, whether or not it would be apparent to anyone at the time, whenever subject-matter described in the prior disclosure is capable of being performed and is such that, if performed, it must result in the patent being infringed, the disclosure condition is satisfied. The flag has been planted, even though the author or maker of the prior art was not aware that he was doing so.
[23] Thus, in Merrell Dow, the ingestion of terfenadine by hay-fever sufferers, which was the subject of prior disclosure, necessarily entailed the making of the patented acid metabolite in their livers. It was therefore an anticipation of the acid metabolite, even though no one was aware that it was being made or even that it existed. But the infringement must be not merely a possible or even likely consequence of performing the invention disclosed by the prior disclosure. It must be necessarily entailed. If there is more than one possible consequence, one cannot say that performing the disclosed invention will infringe. The flag has not been planted on the patented invention, although a person performing the invention disclosed by the prior art may carry it there by accident or (if he is aware of the patented invention) by design."
The 254 Patent
Cribier
- The claimed invention in Cribier is an early version of Dr Cribier's replacement device, i.e. a valve within an anchor or frame. It is discussed mostly for use as a replacement aortic valve, though its placement is not said to be confined to the aorta.
- The issue in relation to novelty was whether Cribier disclosed an apparatus with a fabric seal on the exterior of the anchor which is bunched up in the deployed configuration.
- At p.20-21 Cribier introduces the idea of what is called an 'internal cover' to prevent leakage of blood between the bars of the frame (omitting reference numerals):
"The valvular structure of the invention, as shown in the illustrated example, includes advantageously a third part, i.e., the internal cover to be fixed on the internal wall of the frame. This internal cover prevents any passage of blood through the spaces between the bars of the frame in case the implantable valve would be positioned with the fastening line of the valvular structure on the frame not exactly on the remains of the dilated aortic valve, i.e., either above or below. It also strengthens the fastening of the valvular structure to the frame."
- This is discussed in further detail, partly by reference to figures 6a-c which illustrate alternative embodiments of the internal cover. In each case the cover is exclusively internal. The specification also discusses the internal cover more generally, in particular with regard to the part of the frame below the point at which the valves are fastened (at p.22):
"In other aspects, to prevent any regurgitation of blood from the aorta towards the left ventricle during diastole, the base of the valvular structure is preferably positioned exactly at the level of the aortic annulus against the remains of distorted stenosed valve pushed apart by the inflated balloon. Therefore, there is no possibility of blood passage through the spaces between the metallic frame bars below the attachment of the valvular structure.
However, to avoid any risk of leaks, the part of the frame below the fastening of the valvular structure (about 3 to 5 mm) is preferably covered by an internal cover which is preferably made with the same tissue as the valvular structure. Thus, there would be no regurgitation of blood which is a possibility when there is any space between the valvular structure fastened on the metallic frame and the line of application of the frame on the aortic annulus. The internal cover makes a sort of 'sleeve' below the fastening of the valvular structure on the internal surface of the frame, covering the spaces between the frame bars of the frame at this level, thus preventing any regurgitation of blood through these spaces."
- Here the specification is specifically addressing the regurgitation or leakage of blood in the space between the frame and the annulus. This is prevented by pressing the base of the prosthesis against the native leaflets exactly at the level of the annulus and, by way of further safeguard, the internal cover below the line of fastening of the leaflets forms a 'sleeve' blocking the flow of blood through the frame at this level.
- The specification goes on to disclose the possibility of also having an external cover, although this is confined to the following two sentences (at p.22, here including the reference numerals):
"At Figure 6d, the internal cover 19 is extended at its lower end 19' to an external cover 19" which is rolled up to be applied on the external wall 25 of the stent 10. The internal and external cover are molded, glued or soldered to the bars of the stent 10."
This is figure 6d:
.png)
- No particular function is accorded to the external cover by Cribier. He did not suggest that the external cover should be bunched or otherwise crumpled or folded. The issue was a short one: would the skilled addressee be of the view that if the teaching in Cribier were carried out, the external cover in its deployed configuration would inevitably bunch up and give rise to sealing within the meaning of the 254 Patent? Professor Moore said that bunching and sealing would not be an inevitable consequence. Dr Buller said there would be a degree of crumpling, but not necessarily enough to achieve sealing. On that evidence the 254 Patent does not lack novelty over Cribier.
Bessler
- Bessler claims an invention entitled 'Artificial Heart Valves and Method and Device for Implanting the Same". The valve disclosed is for percutaneous installation following percutaneous ablation of the diseased leaflets. The device has this appearance:
.png)
- Debate again centred on the presence or absence of a bunched up seal in the deployed configuration. Bessler states that the valve has a 'cuff portion', numbered 37 in the figure shown above. He says this (col. 4, lines 4-11):
"The cuff portion of the valve means is attached to the stent member and may extend partly or wholly around the outer perimeter of the stent member. In some of the preferred embodiments of the artificial heart valve of the invention, the cuff portion of the valve means extends on only one side of the circular portion of the stent member."
- Claim 1 of Bessler includes the following integer:
"wherein the cuff portion is configured to position the valve snugly and sealingly at a valve site;"
The suggestion of the cuff forming a seal was not to be found anywhere else in the specification.
- In his first report Dr Buller said that the cuff would typically be made of a synthetic material such as expanded polytetrafluoroethylene (ePTFE) i.e. Teflon, or polyethylene terephthalate (PET). The skilled cardiologist would have realised that as the stent foreshortens, the cuff would tend to bulge outwardly and on deployment longitudinal folds may be present to some extent due to oversizing. In his second report Dr Buller said that the integer in claim 1 quoted above would have led the skilled cardiologist to understand that the intention of the cuff is to fill any gaps or spaces between the outside of the stent and the surrounding native tissue.
- In his first report Professor Fisher said that foreshortening would have been an inevitable consequence of the deployment of Bessler's device. This was not challenged.
- An important part of the idea disclosed by Bessler is that the diseased leaflets were to be percutaneously removed before the replacement valve was installed. It emerged that this has not been achieved even now and such a plan would probably have been viewed with scepticism by the skilled team in December 2003. However, to the extent that anything was made of this, such scepticism could only have relevance to inventive step, not novelty.
- It was put to both Dr Buller and Professor Fisher that the skilled person would have believed that ablation of the leaflets was a pre-requisite to the installation of the Bessler device. Neither accepted this. On the other hand, Dr Buller said that he did not know whether ablation of the leaflets would make the task of sealing easier.
- The question of novelty turns on the cuff. Bessler certainly did not expressly disclose that the cuff could take on a bunched up form in the deployment configuration. Professors Lutter and Moore both interpreted Bessler to mean that the cuff was taut in that configuration. Professor Lutter was not challenged; Professor Moore was challenged on the basis that figures 1-3 of Bessler demonstrated that the cuff was not taut. In my view this was trying to infer too much from what were plainly diagrammatic representations.
- Even on Dr Buller's interpretation of Bessler, two assumptions had to be made before being certain that the cuff was a bunched up seal when the device was deployed. First, that the cuff was made of ePTFE or PET or some other material that lent itself to being bunched up. Secondly that such bunching would provide a seal. The integer in claim 1 of Bessler which I have quoted above suggested that the cuff would act as a seal but this could have been dependent on prior ablation of the native leaflets. As I have said, Dr Buller did not know whether ablation would make sealing easier. Therefore it cannot be said that the cuff would necessarily provide a seal, absent ablation.
- The inferences required to make Bessler anticipate claim 1 of the 254 Patent are not inevitable. Therefore the claims of the 254 Patent do not lack novelty over Bessler.
The 766 Patent
Cribier
- I have found that the external cover disclosed by Cribier would not necessarily bulge out to form a seal. No concept of sacs is disclosed in Cribier and if any were formed, they would not necessarily provide a seal. The claims of the 766 Patent do not lack novelty over Cribier.
Bessler
- The cuff of Bessler consists of only one layer. No sacs could form. None of the claims of the 766 Patent lacks novelty over Bessler.
Seguin
- In closing Mr Acland did not maintain the argument that the 766 Patent was anticipated by Seguin.
Inventive Step
The Law
- The overall principles to be applied when assessing inventive step are well established, see Pozzoli SpA v BDMO SA [2007] EWCA Civ 588; [2007] FSR 37, at [14]-[23].
- A point arose with regard to secondary evidence. In Mölnlycke AB v Procter & Gamble Ltd [1994] R.P.C. 49, Sir Donald Nichols V-C divided the evidence relating to obviousness into that which was primary and that which was secondary (at p.113):
"The primary evidence will be that of properly qualified expert witnesses who will say whether or not in their opinions the relevant step would have been obvious to a skilled man having regard to the state of the art. All other evidence is secondary to that primary evidence."
- He went on to caution against too much weight being given to secondary evidence (at p.113):
"Secondary evidence of this type has its place and the importance, or weight, to be attached to it will vary from case to case. However, such evidence must be kept firmly in its place. It must not be permitted, by reason of its volume and complexity, to obscure the fact that it is no more than an aid in assessing the primary evidence."
- The Vice Chancellor's dual categorisation of evidence relating to inventive step has been referred to frequently since. For example, in Halliburton Energy Services Inc v Smith International (North Sea) Ltd [2005] EWHC 1623 (Pat); [2006] RPC 2, Pumfrey J warned again that secondary evidence can distract attention from the point in issue:
"In the final assessment of a finely balanced argument on obviousness, it is possible that the balance will be tilted in favour of the patent if it is established that many were trying and failing: but this sort of consideration is secondary, and will draw attention away from the main question, which is what is obvious to the skilled person in the light of each cited document, taken separately and interpreted through the eyes of the skilled person. In the usual case, I think, the fact that some investigators tried and failed to solve the problem allegedly solved by the patent is irrelevant to the question with which I am confronted, unless it can be shown that those who failed were aware of the publication under consideration, and the fact of failure will therefore have the strongest effect when the common general knowledge alone is relied on, although even then it must be shown that those who tried and failed were possessed of the common general knowledge and were not the victims of idiosyncratic prejudice or ignorance."
- Later, in Schlumberger Holdings Ltd v Electromagnetic Geoservices AS [2010] EWCA Civ 819; [2010] RPC 33, Jacob LJ (with whom Waller and Sullivan LJJ agreed) considered secondary evidence and its value in some detail:
"[77] It generally only comes into play when one is considering the question 'if it was obvious, why was it not done before?' That question itself can have many answers showing it was nothing to do with the invention, for instance that the prior art said to make the invention obvious was only published shortly before the date of the patent, or that the practical implementation of the patent required other technical developments. But once all other reasons have been discounted and the problem is shown to have been long-standing and solved by the invention, secondary evidence can and often does, play an important role. If a useful development was, in hindsight, seemingly obvious for years and the apparently straightforward technical step from the prior art simply was not taken, then there is likely to have been an invention."
- Jacob LJ considered various types of secondary evidence, including what those skilled in the art thought at the time:
"[81] Another important matter to consider is the reaction of experts at the time of the invention, both before and after. Aldous J. put it this way in Chiron Corp v Organon Teknika Ltd (No. 3) [1994] F.S.R. 202 at 223:
"
it will be necessary to go back to November, 1987 [the priority date] and try to understand the attitudes and thinking of those in the art at the time. That can best be achieved by looking at what was happening and the attitudes of those concerned in the field in the 1980s. Such evidence does, I believe, enable me to decide whether the opinions of the witnesses are consistent with the facts or hindsight reconstructions of the type which are not persuasive."
[82] Whitford J. put it similarly in Joseph Lucas (Batteries) Ltd v Gaedor Ltd [1978] R.P.C. 297, at p.358, lines 79:
"
the question of obviousness is probably best tested, if this be possible, by the guidance given by contemporaneous events."
- Jacob LJ then referred to what Sir Donald Nichols had said in Mölnlycke:
"[85] It would be wrong to read this decision as saying that secondary evidence is always of minor importance. That would be to throw away a vast mass of jurisprudence, including many House of Lords cases, (e.g. Vickers, Sons & Co v Siddell and Technograph). It would indeed involve disregarding some of the approach actually used in Mölnlycke."
Boston's case on the secondary evidence
- Boston's argument with regard to the secondary evidence was simple. It started with the device made by PVT and used by Dr Cribier in his ground-breaking work in 2002. PVT was purchased by Edwards in January 2004. In 2003 or 2004 the next generation in this line of devices was marketed, referred to in the evidence as 'the Cribier-Edwards valve'. Next Edwards marketed the Sapien valve, introduced on to the European market in 2007. This was followed by the Sapien XT and most recently the Sapien 3, first marketed in January 2014. It was not until the Sapien 3 that Edwards used an outer skirt. And in the promotion of the Sapien 3, the outer skirt was advertised as eliminating significant PVL, so the addition of the skirt was apparently seen by Edwards as providing a significant marketing advantage. Boston argued that had the skirt been obvious to the skilled person in December 2003, it would certainly have been equally obvious to Edwards who would then have introduced their skirt a good deal earlier than 2014.
- Boston also pointed out that Dr Cribier himself had continued to work with Edwards as a consultant and had not been asked to give evidence. I was invited to infer that the value of an outer skirt had not occurred to Dr Cribier.
- Dr Buller was cross-examined on this. He agreed that if Edwards had appreciated that there was a tangible clinical benefit to be achieved by including an outer skirt on the Sapien XT, it was incredibly unlikely that this would have been passed up for marketing reasons. He said that he had no knowledge of Edwards' decision making but it would have been a question of weighing up the consequences of modifications to the device and considering what advantage that would give. In re-examination Dr Buller said that a skirt on the Sapien XT would have increased its profile and reduce the number of patients in whom it could be used.
- The expanded and compressed sizes of the Sapien, Sapien XT and Sapien 3 valves were provided in the evidence. These suggested that a Sapien XT with a skirt could have been used on a good proportion of patients and Dr Buller did not suggest otherwise. It was not possible to say what proportion of patients that would have been. But this was a matter on which Edwards could have given evidence had it so chosen. I was left with the impression that a Sapien XT with a skirt would have been appropriate for use in a significant proportion of patients and would have benefited from the marketing advantage of providing the sealing benefits of the skirt.
Edwards' application
- Edwards made an application on the third day of the trial which has some bearing on the secondary evidence. Its origin went back some months. In July 2016 Boston sought disclosure from Edwards. Boston served a witness statement from Michael Burdon of Boston's solicitors ("Olswang") dated 11 July 2016 in which he challenged Edwards to disclose documents, if any existed, showing earlier work done by Edwards on a skirt or other solutions to the problem of PVL. Mr Burdon said that in the absence of such documents Boston would invite the court to draw an inference that it had not been obvious to Edwards at the relevant time to incorporate a skirt on a THV. By implication, Mr Burdon was suggesting that Boston would rely on such an inference in support of their argument that Boston's inventions were not obvious.
- Timothy Powell of Edwards' solicitors ("Powell Gilbert") responded in a witness statement dated 1 September 2016. He said that Edwards did not intend to rely on factual evidence of its own research and that the documents sought would serve no assistance. The assurance that Edwards did not intend to rely on factual evidence of their own research was repeated in a letter dated 8 September 2016.
- It is difficult to see how documents revealing whether or not Edwards had given thought to a skirt on a THV, and if so when, would not be of assistance to the court. It does not follow that Edwards would have been required to give disclosure other factors could have come into play and there has lately been a shift in the tide regarding disclosure in patent actions, see Positec Power Tools (Europe) Ltd v Husqvarna AB [2016] EWHC 1061 (Pat). In any event, Boston did not pursue its application and the parties moved on. Edwards was on notice as to the inference that Boston was going to invite the court to draw and, as was Edwards' right, decided to live with it.
- Then two days before the trial, on 16 January 2017, Powell Gilbert sent a letter stating that they understood from Boston's skeleton that Boston intended to advance an argument based on 'secondary indicia of non-obviousness'. The letter referred to two sentences in the first report of Professor Lutter and one sentence in his second report. Powell Gilbert's letter said that they expected Boston to put their case to Edwards' witness of fact, Russ Joseph. Mr Joseph is Senior Director of Valve Development and Testing at Edwards. He had signed the statement of truth at the end of Edwards' product and process description ("PPD") and was to be made available for cross-examination regarding the PPD, but he had not provided a witness statement.
- I leave aside the suggestion in Powell Gilbert's letter, which cannot have been correct, that Powell Gilbert had only become aware of the argument Boston intended to run because of what Professor Lutter had stated. The more important point, as Mr Meade said when this was raised on the third day of the trial, was that Mr Meade was put into an unfair position. He was being asked to cross-examine Mr Joseph without any idea of what Mr Joseph's views on the topic were. Powell Gilbert's letter sounded very much like an invitation to allow Mr Joseph free rein to give new evidence in cross-examination.
- Mr Acland then adjusted Edwards' position. It became an application by Edwards, on the third day of the trial, to adduce new evidence in the form of a witness statement from Mr Joseph to be served shortly, on which he could be cross-examined. I refused the application and will briefly now give my reasons.
- I cannot rule out the possibility that Mr Joseph was planning to say that Edwards had never thought of the skirt until they became aware of Boston's idea. If so, Edwards were not prejudiced by losing the chance to be so candid. The more likely alternative was that Mr Joseph was going to say that Edwards did think of a skirt for a THV, or some variation on it, and was intending to give reasons why the idea of the skirt was not implemented by Edwards until the Sapien 3. A flavour of what Mr Joseph planned to say came possibly from Edwards' closing submissions (at [13]):
"The question 'if it was obvious why was it not done before?' can play an important role in the overall assessment of obviousness. However, there may be many answers to that question showing that it was nothing to do with the invention, for example because practical implementation of the patent required other technical developments."
- Assuming that Mr Joseph had intended to outline 'other technical developments' required before Edwards could implement the idea of the skirt, Mr Meade would not have been in a position to test the accuracy and completeness of Mr Joseph's evidence regarding what Edwards' valve development team had done. That would only have been possible had Boston's legal team, at least, been given access to Edwards' research documents in due time. Mr Joseph was a technical man, but if he had also been intending to allude to marketing or other commercial factors he felt were relevant, Boston again were entitled to sufficient time to look into such factors in advance of Mr Joseph's giving oral evidence.
- In short, in my view Edwards' application was far too late. Edwards took a strategic decision in August or September 2016 regarding how it was going to deal with Boston's argument on the secondary evidence and non-obviousness in this case, an argument that Boston had clearly signalled. Allowing Edwards to reverse that decision after the trial had started would have resulted in significant unfairness to Boston.
Conclusion on the secondary evidence
- I take the view that on the evidence available, no clear technical reason has been established why Edwards' earlier THVs, in particular the Sapien XT, did not feature an outer skirt of the type subsequently used on the Sapien 3.
- It is relevant that the most important item of prior art in this case is the work done by Dr Cribier which, as is common ground, was known to all in the field in December 2003. Edwards were in that sense in as good a position as the hypothetical skilled person and I have no reason to think that Edwards were at that time victims of idiosyncratic prejudice or ignorance, see Halliburton quoted above. That said, it is also relevant that I have no reason to think that Edwards paid any attention to the cited items of prior art, aside from Cribier.
- Edwards laid emphasis on Jacob LJ's observation that only after alternative reasons why an invention was not done before the priority date can secondary evidence come into play. (He also said that in such a circumstance it can play an important role, see Schlumberger and the passage quoted above).
- I think that alternative reasons for Edwards' failure to use an outer skirt on a THV before the Sapien 3 (i.e. aside from never considering it) have been not been established, bar speculation unsupported by evidence. A credible reason for not adding the skirt earlier is that the addition of the skirt did not occur to Edwards earlier. This in turn generates a suggestion that the use of an outer skirt is not something the skilled person would have considered in December 2003. I find this relevant, but not conclusive. I turn next to the primary evidence and the cited prior art.
The 254 Patent
Cribier
- Edwards said that in December 2003 one of the desirable design criteria for a TAVI device in the mind of the skilled person would have been a means to minimize or eliminate PVL. I agree, although this was only one of a number of possible ways to improve a TAVI device. Edwards further argued that it would have been obvious to the skilled person to adapt the concept of the outer skirt disclosed in figure 6d of Cribier to make a seal. This was based on the following propositions from Edwards:
(i) The skilled team would have appreciated that a frame deployed in a calcified annulus would not form a perfect seal.
(ii) The team could without difficulty have constructed Cribier's outer cover to consist of excess material that would bunch and form a seal in an uneven annulus.
(iii) Alternatively, the most obvious material from which to make the outer cover was PET. The foreshortening of the device would have led the PET to bunch and form a seal.
- Edwards' argument assumes a number of steps taken by the skilled team. First, out of all the ways in which a TAVI device could be improved, the team would focus on reducing PVL. At the time the skilled team would not have viewed the mild PVL reported to be associated with Dr Cribier's valve as being a major threat to the survival of the patient. Secondly, the team would then fasten on to figure 6d of Cribier, a figure to which Cribier attaches no particular significance. I should add that these first two steps are connected. If Cribier had clearly signalled that figure 6d and an outer skirt were of some significance in the reduction of PVL, that could have led the skilled reader to focus on the reduction of PVL as a means to improve a TAVI device. Thirdly, the skilled team would ensure that the outer skirt shown in figure 6d would bunch up and create a seal when deployed. Fourthly, such an arrangement would not be rejected in December 2003 as creating an unacceptably wide delivery profile.
- There is nothing in Cribier that would have motivated the skilled team to take these steps. They would only have been taken if the common general knowledge of the skilled team included the idea that the presence of an outer skirt on the frame would create a seal if it was sufficiently loose so that it could expand out to meet the surrounding vessel wall.
- Had that idea been in the skilled team's mind there were certainly obvious alternative ways to achieve the necessary bunching and sealing, whether by using a non-stretch fabric such as PET plus arranging for foreshortening to happen, or whatever. But the idea in the first place was required.
- Edwards failed to establish that the skilled team's common general knowledge contained this key idea in December 2003. In fact, the evidence pointed the other way. At that time the skilled team would have had firmly in mind the work done by Dr Cribier, providing the only example of a THV that could be successfully implanted in a patient. Dr Cribier's THV had an internal cover but not an external one and this would have provided a powerful guide as to the way forward.
- In closing Edwards relied mostly on the evidence of one of their experts, Professor Fisher. Professor Fisher explained how easy it would be, from his point of view, to implement the external cover shown in figure 6d to make a seal. No doubt. Having improbably focussed on figure 6d in the first place, Professor Fisher apparently thought at once of using the outer cover as an external seal. This was not an idea to be found in Cribier or any other document dating from December 2003 or before. Professor Fisher said that his own thinking reflected what would have been the thinking of the skilled person in 2003. I do not accept that. By 2016 Professor Fisher had had experience of THVs and how they work. He was also uncertain about the sequence in which he had read the documents in this case. In my view the connection which Professor Fisher made between the outer fabric in figure 6d and an external seal for the THV device was the product of well-informed hindsight.
- I think that the same hindsight and/or excess of imaginative skill applied to Dr Buller's view of what the skilled team would have made of figure 6d in December 2003, always assuming they would have given it more than cursory attention. Dr Buller has long been familiar with TAVI devices and how they work and attended a training course on TAVI in New York in 2013. It would be impossible for Dr Buller not to make a connection between an outer cover on the frame of a THV and an external seal to reduce PVL. I was not satisfied that the skilled team in 2003 would make the same connection.
- I find that the 254 Patent does not lack inventive step over Cribier.
Bessler
- In one sense Bessler provides more relevant information than does Cribier. There is the short reference in claim 1 (nowhere else) to the cuff being configured to position the valve snugly and sealingly at a valve site. As against that, an important part of the information that the skilled addressee would take away from Bessler is that the diseased valve should be ablated by percutaneous means in advance of installing the replacement valve. I do not believe that the skilled team would have regarded Bessler as a promising source of information on how to perform a workable TAVI procedure.
- Edwards' argument on Bessler also suffers from a similar difficulty as to that advanced in relation to Cribier. Even assuming that the skilled team would pay particular attention to one integer of claim 1 unexplained in the body of the specification, there is nothing in Bessler to prompt the skilled reader towards the idea of allowing the cuff to provide an external seal by spreading out to reach the vessel wall, particularly at a site still containing diseased leaflets. That idea would not have come from the skilled team's common general knowledge, so it would not have come at all.
- The 254 Patent is not obvious over Bessler.
Thornton
- Thornton is a US patent for an invention entitled 'Endolumenal stent-graft with leak-resistant seal'. It is not concerned with heart valves but with an endograft used to treat an abdominal aortic aneurysm ("AAA"). An AAA is an enlargement of the abdominal section of the aorta. As the diameter of the aorta enlarges, its wall becomes thinner and if left untreated it may eventually burst, typically leading to the death of the patient within a few minutes.
- An endograft is a stent covered with graft material on the internal or external surface. It can be introduced percutaneously into the aorta at the site of the aneurysm. Once securely anchored at either end of the aneurysm, it replaces that part of the artery so that the blood flowing within it exerts no radial pressure on the weakened section of the artery wall. Relieving the aneurysm of pressure will happen only if the endograft is sufficiently well sealed at either end so that it does not migrate and, importantly, so that blood does not leak into the part of the artery with the weakened wall.
- There are two methods of sealing disclosed. Edwards focussed on the first, which is shown in figure 1 of Thornton. Figure 1 is reproduced below followed by part of its description in the specification (at col. 7, lines 43-56):
.png)
"More particularly in FIG. 1, flange (26) is shown in a flared condition, which condition may be its relaxed geometry or may be a geometry imparted thereto by flow in the occluded direction. In the case where the flared shape of flange (26) is its relaxed geometry, flange (26) may include an outward bias to that shape, such that when tubular member (10) is deployed into an endolumenal space (not shown in FIG. 1), flange (26) may engage a radially confining endolumenal wall defining that space (not shown) and thereby enhance the reduction of flow around tubular member (10) between outer surface (18) and the endolumenal wall."
- The specification states that the seal disclosed (in the figure 1 embodiment, the flange) may be used in various forms in implantable endovascular medical devices generally (col. 8, lines 32-47):
"While particular variations of the seal member of the present invention are herein described such as in FIGS. 1 and 2, it is to be further appreciated by one of ordinary skill that other seal member variations may be secured to outer surfaces of implantable endovascular medical devices without departing from the scope of the invention. For example, a thrombogenic material such as collagen or Dacron fibers may be secured to an outer surface of an implantable endolumenal medical device and suitably occlude flow around that device for a particular medical application. However, clinical limitations, such as profile, lubricity, traumaticity, or toxicity may dictate the utility of a particular seal member when it is intended to be combined with a tubular member which is designed for a particular application."
- By way of alternative to collagen or Dacron (PET), in at least one embodiment a thin-walled ePTFE tape is also proposed as a material generally to be used for the seal member, which should be as thin as possible to functionally provide a flange-one-way-valve function (col. 29, lines 17-19)). Use of thin ePTFE was particularly relied on by Edwards. There was a dispute about its suitability for use as a seal in a THV, which I will come to, but no dispute that the skilled addressee would understand that it was a material which could be used for the flange in figure 1 of Thornton.
- Edwards' argument was that it would have been obvious to the skilled team to use a flange seal of the type disclosed in Thornton to prevent leakage around a THV. This would have been a THV of the type used by Dr Cribier and disclosed in the 2002 Cribier Paper and in Dalby. Such a flange would in its deployed state have taken the form of a bunched up fabric seal as required by claim 1 of the 254 Patent.
- In his first report Dr Buller said that Thornton would be of real interest to the skilled cardiologist in the team. The seal proposed is simple and the skilled cardiologist would find it obvious to position the Thornton seal so that it would work on a THV. Specifically, it would extend from the distal end of the skirt. He provided a diagram and annotation to show what he meant:
.png)
Figure 32: Example of a Thornton seal combined with a THV, showing the seal (red), skirt (blue), stent (black) and valve (green)
- Dr Buller added that the skilled cardiologist would appreciate that the backflow of blood (in Dr Buller's diagram above this would be in the downward direction) would fill the Thornton seal, causing it to compress downwards, bulge outwards and conform to irregularities in the surrounding tissue.
- Professors Moore and Lutter raised a number of obstacles in the way of using Thornton's seal on a THV. First, the skilled team interested in TAVI devices would not expect to find useful ideas in a patent about endografts. Second, stents are anchored against healthy, elastic parts of the aorta rather than having to cope with calcified walls and native leaflets. Third, the flange appears to be stiff as shown in figure 1 of Thornton. Fourth, the flange would have taken up a lot of space and therefore compromised the delivery profile. Fifth, a soft material would not press firmly against the artery wall to form a seal. Sixth, Thornton teaches that wrinkles cause leaks, which is the opposite of the wrinkling and bunching of the seal taught in the 254 Patent. Seventh, there was a risk that the flange might obstruct the coronary ostia.
- It seemed to me that in his second report Dr Buller provided answers to all these points, which he maintained convincingly in cross-examination. First, Dr Buller said he totally disagreed with the idea that the skilled team would not expect to find useful ideas in Thornton. He said that teachings about TAVI devices had often referred to TAVI as an extension of endograft concepts. Second, it was well known that points of attachment of a stent proximal and distal of the aneurysm were frequently irregular and calcified. Third, the stiff appearance of the flange in the figures of Thornton is only a diagrammatic representation; ePTFE would not maintain a stiff cone shape in use. Fourth, ePTFE tape is 0.1mm thick or less, so even in its delivery configuration would not take up significant space. Fifth, the ePTFE would consist of excess material in the delivery mode, which would expand into a flange when blood was caught in it and be forced against the vessel wall. Sixth, the wrinkling warned against in Thornton concerns the tubular cover of the stent, where wrinkling may be caused by under-expansion of the stent. The flange will seal leaks due to such wrinkles by bulging outwards and conforming to the irregularities in the surrounding tissue. Seventh, if the Thornton seal were placed at the bottom of the stent, as shown in Dr Buller's diagram above, it would not block the coronary ostia.
- In cross-examination Dr Buller was asked to, and did, make drawings to illustrate further how a Thornton flange would behave in use on Cribier prior art THV.
- Mr Acland elected to cross-examine Professor Moore rather than Professor Lutter on Thornton and indeed the rest of the prior art. As I have indicated, Professor Moore's evidence was generally a good deal less compelling than that of Dr Buller. Professor Moore was cross-examined at considerable length on Thornton. In my view, part of the reason the cross-examination stretched out so long was that Professor Moore tended to deploy being obtuse as a means of avoiding direct and clear answers.
- The main points made by Professor Moore in cross-examination were firstly that a seal of ePTFE would be 'smashed' between the endograft and the vessel wall and would not flare out, although later it emerged that all he meant by this was that it would be pinned between the endograft and the wall. Secondly the skilled team would not use enough tape for it to reach the vessel wall this is hard to reconcile with the first point. Thirdly, it would increase the delivery profile of a THV, although I did not understand Professor Moore to say that this would make it a THV with such a seal impractical for use in any clinical context.
- I prefer the evidence of Dr Buller. The skilled team would have been interested in a general way in anything that might improve the performance of Dr Cribier's THV, which was part of their common general knowledge. Reducing PVL would be only one of several means of making such an improvement, but it would nonetheless have been in the mind of the skilled team in December 2003. The hypothesis is that the team was given a copy of Thornton and read it with interest. They would have regarded it as having come from a field related to TAVI. They would have been aware that the seals used for endografts treating AAA must be particularly effective because a leak in the endograft is liable to be fatal. The flange in Thornton is clearly shown in figure 1 and discussed as a seal in some detail in the specification. In my view the skilled team would have thought it obvious to try using the Thornton flange as a seal on a THV in the manner described by Dr Buller, with a reasonable expectation of success by which I mean an expectation of reducing PVL to a significant extent. Had that been done, the excess of fabric towards the unattached end of the seal would have caused it to fold in deployment and consequently to become bunched up according to the construction of that term I have reached above. The blood flow would have caused the fabric to bulge out and lie adjacent to the vessel wall, conforming with its contours, thus preventing blood flow past the THV to significant extent.
- In closing Mr Meade pointed out that Mr Acland had not cross-examined Professor Lutter on the prior art, save for a short question on Seguin. Mr Meade said that if an invention was not obvious to one member of the skilled team over the prior art, then in law it was not obvious. (This was leaving aside the unusual circumstance in which one member of the team addressed, say, inventive step and another sufficiency, see Schlumberger, cited above).
- I think this was putting the matter too simply. The present case is an example of the frequent circumstance in which there is overlap between the circles of expertise of the members of the skilled team, to use a Venn diagram image. Mr Meade's point would have been a good one if Professor Lutter had raised a reason why the invention in the 254 Patent would not have been regarded as obvious to a skilled interventional cardiologist and that reason was plainly solely within the latter's circle of expertise. In my view that did not apply to the present case.
- Before leaving Thornton I should add one further matter. Edwards argument on obviousness over Thornton was based, as I have explained, on Dr Buller's evidence and his diagram of how a Thornton flange would be used as a seal figure 32 from his first report, shown above. As Dr Buller said (at [179]) and as that diagram shows, the seal extends from the distal end of the (inner) skirt, not the distal end of the valve as required by claim 1 of the 254 Patent. This was not a point raised by either side, I assume because it was jointly seen as irrelevant. I mention this because it reinforces the view I have taken on the construction of claim 1 of the 254 Patent, regarding the lack of importance which the skilled team would have attached to any precise connection between the positioning of the fabric on the outside of the anchor and the point of attachment of the leaflets on the inside.
The 766 Patent
Cribier
- Edwards' argument on Cribier and inventive step suffers from a flaw similar to that which applies to Edwards' equivalent argument in relation to the 254 Patent. Nothing in Cribier would prompt the skilled to team to focus on figure 6d, consider how it might be adapted to reduce PVL, make a sac and ensure that it would create a seal when deployed.
- The common general knowledge of the skilled team would not have made up for this deficiency. The 766 Patent does not lack inventive step over Cribier.
Bessler
- For reasons explained above, there is nothing in Bessler to prompt the skilled reader towards the idea of allowing the cuff to provide an external seal by spreading out to reach the vessel wall, particularly at a site still containing diseased leaflets. Even less is there anything in Bessler to suggest that this should be achieved by using a two-walled sac. The 766 Patent is not obvious over Bessler.
Thornton
- I have found that that the invention claimed in the 254 Patent is obvious over Thornton. The important difference between that invention and the one claimed in the 766 Patent is that the latter requires a sac and therefore a cavity with two walls. Nothing in Thornton teaches the further step of creating a sac and nothing in the skilled team's common general knowledge would have led the team towards using a sac as a seal. The 766 Patent is not obvious over Thornton.
Seguin
- Seguin was only relied on in support of Edwards' argument that the invention claimed in the 766 Patent was obvious. It is an international patent application for an invention entitled 'Tubular support for setting, by percutaneous route, a substitution cusp'. The 'substitution cusp' (translated from the French) is a replacement valve.
- Seen from the side, Seguin's support structure comprises a central 'valve support portion' and at least one 'wedging portion' above or below the axial portion. The wedging portion(s) have a diameter greater than that of the axial portion and support the structure against the vessel wall. The axial portion supports the valve.
- The support structure has an expanded form for use once the device is in place in the annulus and a compressed form for insertion into a catheter. These are shown in end view respectively in figures 3 and 4. On page 6 of the translation the specification introduces the idea of a seal:
"Advantageously, the axial valve support portion includes, at its outer face, sealing means configured so as to absorb the surface irregularities that may exist at or near the remaining cardiac annulus."
- Four forms of sealing means are described, each of which consists of material on the periphery of the stent. They are illustrated in figures 17-21 (the fourth embodiment is shown in two phases). In closing Edwards relied only on the version shown in figure 19, in which 1 is the axial support, 6 is a peripheral strip. Between this and the annulus 10 there is a further strip 8:
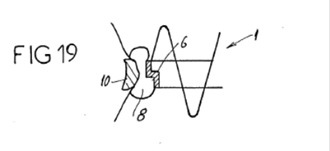
Strip 8 is described as follows:
"This strip 8 defines a chamber and has a radially expandable structure, such that it has, in cross-section and in the inflated state, two widened ends protruding on either side of the strip 6. This chamber can receive an inflating fluid able to congeal within a predetermined length of time after insertion into said chamber. Once this material is congealed, the inflating catheter is sectioned."
- Edwards argued that the idea of the inflatable strip would be appreciated by the skilled team and incorporated into a Cribier THV to create a sac within the meaning of claim 1 of the 766 Patent. The argument was supported by their experts in their respective reports, but less so in cross-examination. Dr Buller described the general teaching of Seguin, particularly by reference to figures 3 and 4, as unrealistic, unfeasible and a very bad idea. Professor Fisher said that more work needed to be done and that the patent had not demonstrated the idea to be feasible.
- Even assuming the skilled team was undeterred by the general teaching and zeroed in on the idea shown in figure 19 though there was no reason to suppose that it would have done this too lacked credibility. Dr Buller said that band 6 as shown in figure 19 was a very bad idea. Professor Fisher said that the concepts shown in each of figures 17-21 needed further engineering design work.
- I find that the 766 Patent does not lack inventive step over Seguin.
Insufficiency
- Edwards' argument on insufficiency was that insofar as Boston contended that the inventions claimed in the Patents were not obvious because the skilled team would have been deterred from using the skirt idea, since it would add to the delivery profile of the device, neither Patent disclosed how to circumvent this difficulty.
- First, Boston's arguments did not hinge on delivery profile. Secondly, even if they had and to the extent that delivery profile was discussed, it does not follow that the Patents failed sufficiently to disclose the inventions. It was not suggested that the skilled team would be unable to perform the inventions having read the Patents. If the skilled team had laboured under a technical prejudice in December 2003 regarding delivery profile, it would have been removed by the teaching of the Patents.
Added Matter
- The Re-Re-Re-Re-Amended Grounds of Invalidity plead two overall arguments of added matter against both Patents. In each case the first is an allegation of the claims of the granted Patent consisting of intermediate generalisations; the second is a more straightforward allegation that claims disclose matter nowhere disclosed in the Application.
The law
- Kitchin LJ (with whom Laws and Etherton LJJ agreed) explained the concept of intermediate generalisations in Nokia Corporation v IPCom GmbH & Co KG [2012] EWCA Civ 567; [2013] RPC 5. This was in the context of a proposed amendment to claims. He said:
"[56] Turning to intermediate generalisation, this occurs when a feature is taken from a specific embodiment, stripped of its context and then introduced into the claim in circumstances where it would not be apparent to the skilled person that it has any general applicability to the invention.
[57] Particular care must be taken when a claim is restricted to some but not all of the features of a preferred embodiment, as the TBA explained in decision T 0025/03 at point 3.3:
"According to the established case law of the boards of appeal, if a claim is restricted to a preferred embodiment, it is normally not admissible under Art.123(2) EPC to extract isolated features from a set of features which have originally been disclosed in combination for that embodiment. Such kind of amendment would only be justified in the absence of any clearly recognisable functional or structural relationship among said features (see e.g. T 1067/97, point 2.1.3)."
[58] So also, in decision T 0284/94, Neopost/Thermal Printing Mechanism [2000] E.P.O.R. 24, the TBA explained at points 2.1.3-2.1.5 that a careful examination is necessary to establish whether the incorporation into a claim of isolated technical features, having a literal basis of disclosure but in a specific technical context, results in a combination of technical features which is clearly derivable from the application as filed, and the technical function of which contributes to the solution of a recognisable problem. Moreover, it must be clear beyond doubt that the subject matter of the amended claim provides a complete solution to a technical problem unambiguously recognisable from the application.
[59] It follows that it is not permissible to introduce into a claim a feature taken from a specific embodiment unless the skilled person would understand that the other features of the embodiment are not necessary to carry out the claimed invention. Put another way, it must be apparent to the skilled person that the selected feature is generally applicable to the claimed invention absent the other features of that embodiment.
[60] Ultimately the key question is once again whether the amendment presents the skilled person with new information about the invention which is not directly and unambiguously apparent from the original disclosure. If it does then the amendment is not permissible."
- All of Edwards' arguments are based on the allegation that there are disclosures in claims of the granted Patents which cannot be found in the Application. The short answer to this might be that the primary purpose of a claim is to define the patentee's monopoly, not disclose subject-matter. If the claims in question do not mention the additional subject-matter relied on, they cannot have disclosed it. See, for example, Napp Pharmaceutical Holdings Ltd v Ratiopharm GmbH [2009] EWCA Civ 252; [2009] RPC 18, at [98]-[99].
- This reasoning would deal with Edwards' arguments in short order, but I am not certain that it is open to me to stop there. The law on added matter was recently reviewed by Floyd LJ (with whom Longmore and Lewison LJJ agreed) in AP Racing Ltd v Alcon Components Ltd [2014] EWCA Civ 40; [2014] RPC 27. The patent concerned brake calipers used in racing cars. The invention was the incorporation of 'peripheral stiffening bands' or 'PSBs' into the structure of the calipers. One of the integers of claim 1, referred to below by Floyd LJ as feature (6), required that the PSBs should be assymetric (about a lateral axis of the caliper when viewed in plan). Floyd LJ said:
"[28] The passage on p.4 of the application is, to my mind, a clear disclosure of a class of configurations of PSB which are in fact asymmetric about a lateral axis. The teaching of the document is that the PSB follows the outer lateral edge of the limb and turns around the corner to follow the leading or trailing edge as appropriate. The application thus contains a clear and unambiguous disclosure of a class of PSBs which would fall within claim 1 of the granted patent because they would necessarily possess all the features of that claim, including feature (6).
[29] Is the patent nevertheless bad for added matter because it claims a wider class of asymmetric PSBs than are disclosed in the application? The judge thought it did because it claimed all asymmetric PSBs and not just hockey stick shaped ones. Whether he was right depends on an analysis of the extent to which it is legitimate to add features to a claim which describe the invention in more general terms than a specific embodiment.
[30] There is no doubt that the claims of the patent form part of the disclosure for the purposes of assessing whether there is added matter. However the claims perform a different function from the disclosure in the body of the specification. The primary function of the claims is to delimit the area of the patentee's monopoly. Thus in Texas Iron Works Inc's Patent [2000] R.P.C. 207 the patentee had disclosed 'slips and cones' which acted as hanger units in an oil well hanger. In the granted patent the patentee coined the phrase 'liner hanger unit' to define his monopoly, although the phrase was apt to cover units other than slips and cones. Aldous LJ. (with whom Simon Brown and Mantell LJJ. agreed) said this at p.245:
"
the purpose of the claims in a patent is the identification of the ambit of the protection and disclosures are normally a matter for the specification. The application before the amendment clearly and ambiguously disclosed slips and cones which acted as hanger units. The amendment did not alter that disclosure. By using the phrase "liner hanger unit" in the claim the patentee did not disclose any other construction of liner hanger: the term was used to widen the ambit of the monopoly."
[31] In AC. Edwards Ltd v Acme Signs & Displays Ltd [1992] R.P.C. 131 it was argued that three features of a claim of the granted patent were stated in more general terms than the disclosure of the specific embodiment. Thus, for example, the application disclosed the use of a coil spring and cotter arrangement as a retaining means, but the relevant added feature simply specified a 'spring means' Fox LJ. (with whom Staughton LJ. and Sir Michael Kerr agreed) concluded that this did not add matter. Fox LJ. said:
"
claims, as a source of disclosure, have no greater force than the other admissible documents
Mr Whittle is, I think, correct when he says that the claim covers those matters because the patentee chose to limit its claim by reference to features other than the three in question. In practical terms I do not think there is anything very surprising about that result since the purpose of the claims is the identification of the ambit of protection. Disclosures are normally a matter for the specification. One looks, no doubt, at the whole of the issued patent specification in determining what it discloses, but even so, I find no disclosure in claim 1."
[32] In Decision T 0653/03, Toyota Jidosha KK, 8 April 2005 (unreported), the Technical Board of Appeal of the European Patent Office concluded that the replacement of the term 'diesel engine' by the term 'combustion engine' in a claim to a method of purifying exhaust gas constituted added matter. The Board concluded that the disclosure of the granted patent would be understood to mean that the method of the invention was suitable for any type of engine, not merely diesel engines, and that such a teaching could not be derived from the application as filed.
[33] It is clear from these decisions that the law does not prohibit the addition of claim features which state in more general terms that which is described in the specification. What the law prohibits is the disclosure of new information about the invention. In the Toyota case there was such a disclosure of new information, namely the new information that the invention was suitable for engines other than diesel engines. However in Texas Iron Works and A. C. Edwards the specification and claims when read together did not disclose any new technical information, despite the generalisation involved in the added claim feature."
- At this point in the judgment it might appear the Court of Appeal was endorsing without qualification the reasoning set out in earlier judgments, in particular Texas Iron Works and A.C. Edwards, also Napp: the criterion to be applied in determining whether a claim of itself discloses added matter is whether the claim mentions the alleged added subject-matter. On the other hand, in Toyota there was a finding that added matter had been disclosed. This was apparently also a case in which the added subject-matter in question was said to have been disclosed in a claim. Yet it is not clear that the granted claim mentioned types of combustion engine other than diesel engines. Toyota is unreported, but referred to in Case Law of the Boards of Appeal of the European Patent Office, 8th ed. The editors say this about T 653/03 at p.438:
"In T 653/03, the original term 'diesel engine' in claim 1 was replaced by the term 'combustion engine'. Thus the suitability of the claimed method was generalised to any type of combustion engine. The board decided that the treatment of exhaust gas in the original application was always related to a diesel engine, and it could not be inferred by the skilled person that the subject-matter of the granted patent extended to a method which was suitable for any type of combustion engine. The technical contribution was that the amended method was suitable for any type of combustion engine, whereas in the original form it was suitable only for a diesel engine. The generalisation was not admissible."
- Floyd LJ went on to say this in AP Racing:
"[40] In my judgment, the judge's conclusion on this issue was wrong. Having correctly concluded that the description in the application of the hockey stick shaped PSBs was of something 'necessarily asymmetrical' he should have gone on to ask himself whether there was any added disclosure in the granted specification. The description of the PSBs in claim 1 as 'asymmetric' has to be read as part of the disclosure of the specification of the granted patent as a whole, taking account of the different function of the claims and the specification. When this is done the skilled person would understand that the patentee has drafted his claim so that it covers asymmetric PSBs generally. However I am not persuaded that the specification read as a whole discloses any configuration of PSB which is not disclosed in the application. The skilled person would understand from the granted patent, just as in the case of the application, that the PSBs disclosed include those which follow a lateral and leading edge (and therefore are asymmetrical about the lateral axis). The skilled person would also understand that the PSBs are exemplified by the hockey stick shapes described in the specific embodiments. He or she would not, therefore, learn any new information about the invention."
- I interpret this paragraph to mean that if the skilled person reading the application as filed would understand that the narrower class disclosed exemplifies a broader class, then a claim in the granted patent to the broader class discloses no new technical information and does not offend the prohibition against added matter. On the other hand, if the skilled person would not have that understanding and the broader class is not otherwise disclosed in the application as filed, the court is liable to conclude that a claim to the broader class in the granted patent constitutes a disclosure of added matter.
- I will consider whether the relevant claims of the Patents in the present case disclose new technical information over and above that disclosed in the Application. For simplicity of discussion, I will assume that a claim covering an embodiment would imply to the skilled addressee that the invention as disclosed in the Patent includes such an embodiment.
The Application
- The Patents share the same application as filed: PCT/US/2004/043607 ("the Application").
The 254 Patent
- The first of the two overall allegations starts with the proposition that the apparatus claimed in the 254 Patent is disclosed in the Application in two embodiments:
(i) as depicted in figures 32-34 and described at p.34, lines 26-31 and p.86, lines 22-32 ("the Fig 32-34 Embodiment"); and
(ii) as depicted in figures 107A-107C and described at p.84, line 30 to p.86, line 2 ("the Fig 107 Embodiment").
- The pleading goes on to allege that every claim of the 254 Patent comprises combinations of features which differ from the combinations shown in either of the two expressly disclosed embodiments and that the significance of the features selected for each of the claims would only be understood in the context of either the Fig 32-34 Embodiment or the Fig 107 Embodiment. Therefore each of the claims in the Patent amounts to an invalid intermediate generalisation.
- The second argument is that is that the Application nowhere discloses that the fabric seal may bunch up only in response to backflow blood pressure. This is what is claimed and disclosed in claim 6, so claim 6 discloses added matter.
'Wherein the seal is bunched up in the deployed configuration'
- Edwards' first specific argument is that there is no disclosure in the Application that there can be bunching up of the seal in the deployed configuration without this being caused by foreshortening, although such a possibility is covered by claim 1.
- Boston directed my attention to the passage of the Application at p.34, lines 26-31 (omitting figure numbers):
"Figures 32-34 show another way to seal the replacement valve against leakage. A fabric seal extends from the distal end of the valve and back proximally over anchor during delivery. When deployed, as shown in Figures 33 and 34, fabric seal bunches up to create fabric flaps and pockets that extend into spaces formed by the native valve leaflets, particularly when the pockets are filled with blood in response to backflow blood pressure. This arrangement creates a seal around the replacement valve."
- Edwards argued that figures 32-34 (they are shown at paragraph 102 above as figures 22-24 of the 254 Patent) would indicate to the skilled team that the seal is only bunched up in the deployed configuration and the figures show foreshortening to have occurred in that configuration. In my view this is giving too much weight to diagrammatic representations. The passage above discloses bunching up of the fabric seal without any mention of foreshortening. A later passage in the Application, at p.86, lines 22-32, again refers to figures 32-34 and here speaks of foreshortening during deployment for that embodiment. I think the skilled team, having read both passages, would understand that the foreshortening is optional. Bunching can be present with or without it. It was clear from the evidence that the skilled team's common general knowledge would include an understanding that foreshortening of a THV was optional and usually undesirable (see above).
- I do not believe that the skilled team, having read the Application, would think that there is any necessary connection between bunching and foreshortening. Bunching could be present in the delivery configuration and would remain in the deployed configuration. The claims add no new technical information in this regard.
Flaps, pockets and pleats
- Edwards argued that the Application disclosed bunching up of the seal only in connection with the creation of flaps, pockets and pleats. Claim 1 discloses bunching with any result and therefore added matter.
- The Application discloses the creation of flaps and pockets, or pleats, and in my view the skilled team would understand this to mean the folding of the fabric seal in various ways, which is a necessary consequence of there being excess fabric. This is also what is meant by 'bunching up'. In other words, the term 'bunching up' used by itself connotes exactly the same thing. No added technical information is disclosed in claim 1.
Claim 6: backflow blood pressure
- Edwards referred to two passages in the Application in which it is stated that the fabric seal bunches up particularly when the pockets are filled with blood in response to backflow blood pressure. It was argued that claim 6 discloses the seal bunching up solely in response to backflow blood pressure and that this adds matter.
- I do not agree. The skilled team would understand the Application to mean that one possible reason for the seal bunching up is that it does so only in response to backflow blood pressure. There is no new technical information in claim 6.
The 766 Patent
- Edwards' first argument under this head depended on the assumption that Boston's case on a correct construction of claim 1 was that the sac did not include a front and back wall. I did not understand this to have been Boston's argument and in any event it is not how I have construed the term 'sac'.
- The second argument was that the skilled team would understand that the means filling the sacs as illustrated in figure 14, the location of the sacs shown in figure 15 and the details of slots, pores and openings in the sacs shown in figure 16 are all features which have a technical connection with the function of the sacs. Claim 1 discloses a sac generally without those features and so adds matter.
- In my view the skilled team would clearly understand from the specification as a whole that the figures referred to merely illustrate possible ways in which the sac can be filled, located or structured. There may be others. Claim 1 adds no new information.
- The third argument was a variation on the first. It was that insofar as the claims of the 766 Patent cover apparatus with sacs that are combined with another structure or component to provide a seal, this is not disclosed in the Application.
- The skilled team would have understood from the Application that there will be a variety of alternative ways in which the sacs may be combined with other structures or components. To the extent that such alternatives are claimed, this is not a disclosure of new technical information.
Conclusion
- The 254 Patent is invalid on the ground that it lacks inventive step. Had it been valid, it would have been infringed. The 766 Patent is valid and infringed.
Post Script
- After a draft of this judgment was provided to counsel, in a Note dated 1 March 2017 Boston's counsel asked me to give judgment in relation to the validity of claims 2-6, 9 of the 254 Patent in the light of my finding that claim 1 lacked inventive step over Thornton. It was pointed out that these were all alleged to be independently valid claims in Boston's Re-Amended Notice of Independently Valid Claims and that the allegation was maintained in their written closing submissions. I was also reminded that Edwards in the end did not challenge the validity of claim 13.
- In response, Edwards' solicitors pointed out that Boston had not raised any distinct arguments in respect of these other claims in relation to Thornton.
- I think that Boston is entitled to have my view on the validity of claims 2-6, 9 and 13, which I will state briefly. Boston's counsel argued in their Note that my finding that claim 1 lacks inventive step combined with my finding that claim 3 is not infringed, and the reasons I gave for that, suggested that the skilled team would not have thought it obvious to create a device with pleats within the meaning of claim 3, 4 or 5.
- I accept that argument. Starting with Thornton, at the priority date I doubt that the skilled team would have considered a fabric seal which bunched up into pleats in the deployed configuration. If they did, it would have been seen as an awkward refinement, conferring no advantage over irregular folds. Claims 3-5 do not lack inventive step. Claims 6 and 9 do not lack inventive step in so far as they are dependent on claims 3-5.
- Edwards did not maintain its challenge to validity of claim 13 and therefore I find that claim 13 is valid.
- None of the foregoing alters the conclusion given in paragraph 250 above.
