Mr Justice Mellor:
INTRODUCTION.. 4
TECHNICAL BACKGROUND.. 5
Anatomy of the eye - general information.. 5
The functioning of a healthy eye. 8
Cataract surgery - general.. 9
Initial Corneal Incision. 10
Anterior Capsulotomy. 11
Lens Removal 11
Implantation of IOL. 12
Possibility of posterior capsulotomy following cataract surgery. 13
Typical dimensions in the adult eye. 13
Laser technology - general.. 13
Laser gain media. 15
Continuous wave and pulsed laser operation. 16
Gaussian beam optics. 18
Components of laser and optical systems. 19
Lenses. 19
Galvanometric mirrors 21
Beam splitters / Beam combiners 21
Laser-tissue interaction.. 22
Photochemical interaction. 22
Photothermal interaction. 22
Photoablation. 23
Photodisruption. 23
Femtosecond Lasers. 24
Imaging techniques. 25
Confocal microscopy. 26
Optical coherence tomography (OCT) 27
Confocal Microscopy and OCT in context 30
Fluorescence and multiphoton fluorescence. 31
The Patents. 32
The characteristics of the laser. 33
The capability of the imaging system(s) 35
The capability of the control system(s) 42
Conclusions as to the CGK assumed by the Patents. 42
The claims of EP861. 45
The claims of EP528. 47
The expert witnesses. 49
The Skilled Team... 50
CGK.. 59
Introduction to the CGK topics which remained in dispute. 59
CGK - applicable legal principles. 61
Application of the principles in this case.. 63
1. Sources of CGK.. 63
2. The nature of this field. 66
3. The perceived need to improve cataract surgery: anterior capsulotomy & lens fragmentation. 67
4. Refractive surgery and femto-LASIK. 70
5. The use of lasers in ophthalmology. 72
6. Turnkey femtosecond lasers. 77
7. OCT and its use in ophthalmic applications. 77
8. The Skilled Engineer’s knowledge of OCT. 79
9. Control of lasers used in ophthalmology. 80
VALIDITY.. 83
Applicable principles. 83
The Prior Art.. 84
Freedman.. 84
Disclosure.. 84
Obviousness over Freedman.. 90
Mühlhoff.. 93
The nature of the disputes over Mühlhoff. 93
The disclosure of Mühlhoff. 93
My decisions on the disputes over the disclosure of Mühlhoff. 102
Obviousness over Mühlhoff. 110
The first embodiment 111
The fifth embodiment 115
Insufficiency.. 119
Conclusions. 120
1. This case concerns two patents for ophthalmic surgical systems for carrying out cataract surgery, each with a priority date of 10 January 2005. Cataract surgery is one of the most commonly performed eye operations. At the priority date around 9.1 million cases were performed annually worldwide, with 2.5m in the US and around 300,000 cases in the UK.
2. The two patents in suit are EP(UK) 1 835 861 B2 (EP861), entitled “Apparatus for Patterned Plasma-mediated Laser Trephination of the Lens Capsule” and EP(UK) 2 548 528 B1 (EP528), entitled “Apparatus for Patterned Plasma-mediated Laser Trephination of the Lens Capsule and Three-dimensional Phaco-Segmentation”. EP528 is a divisional of EP861. Their specifications are materially identical. Both claim a system comprising a laser and an imaging device for carrying out a surgical procedure on the eye. The primary difference between them is in their specific application: the claims of EP861 are to the device for performing an anterior capsulotomy (AC) (i.e. cutting the anterior lens capsule); the claims of EP528 are to the device for cutting the lens cortex and nucleus into fragments - lens fragmentation (LF). In both Patents, the imaging device is either an Optical Coherence Tomography (OCT) device or a confocal microscope.
3. Thus, the Patents and this case require an understanding of (a) the structure of the eye; (b) the state of the art surgical procedures on the eye, including in particular, the procedures within cataract surgery of performing an anterior capsulotomy and lens fragmentation and removal, but also other procedures such as radial keratotomy; (c) the use of lasers in such surgical procedures and (d) imaging techniques suitable for use on tissues in the eye, including in particular OCT and confocal microscopy.
4. Both patents are owned by the Defendant (AMO). The claim was initially brought by the Claimants (Alcon) seeking revocation of EP861. AMO counterclaimed for infringement and stated its intention to allege infringement of EP528 as well. In due course, claims for revocation and infringement of EP528 were added.
5. Alcon’s Grounds of Invalidity originally challenged the priority date of each patent, alleged lack of inventive step over two pieces of prior art called Freedman and Mühlhoff and included various insufficiency allegations.
6. Alcon now accepts that its LenSx laser surgery system infringes both Patents if they are valid. Alcon has also dropped its challenge to priority. The insufficiency allegations were retained ‘as a squeeze against obviousness’ but were said by Alcon to have done their job, in the sense that the experts are agreed that the skilled team could put the claimed inventions into effect without undue burden. For this reason, the live issues at trial were obviousness over Freedman and Mühlhoff and almost nothing was said about insufficiency. However, for reasons which I explain below, insufficiency has become a point of some significance.
7. The parties were agreed that the Skilled Team would comprise a Skilled Ophthalmologist (SO) and a Skilled Engineer (SE). At the trial the major disputes centred on the characteristics of those members of the Skilled Team and their CGK, which in turn fed into major differences of interpretation of each piece of prior art. In view of the range and number of points in dispute, the trial was overly compressed.
8. The parties had agreed a Technical Primer before the PTR, but it did not purport to record all the CGK or any of the CGK disputes. At the PTR I was persuaded to try, by way of an experiment, a procedure whereby the parties would attempt to compile a Statement of Agreed CGK together with a list of CGK issues in dispute after trial. In retrospect, this was a mistake. It would have been better if I had made an Order at the PTR which kept the pressure on the parties (and in particular AMO) to define their positions on CGK before trial. When I received the written closings, Alcon appended what they proposed as constituting CGK. AMO explained their position on the points in dispute.
9. Notwithstanding those observations, after trial I did receive a Statement of Agreed CGK plus a list, with cross-references to the written and oral evidence, of CGK issues in dispute. This was a helpful document and I am very grateful for the work done in preparing that document. The Technical Background section which follows is very largely based on that document.
10. A cross-section of the human eye is shown in Figure 1 below. Descriptions of parts of the eye are set out further below, arranged alphabetically. The terms “anterior” and “posterior” are used to denote the relative position of structures within the eye. Typically, “anterior” refers to something closer to the front of the eye (toward the left in Figure 1) whilst “posterior” refers to something closer to back of the eye (toward the right in Figure 1).
11. Different elements of the eye have different properties, including different refractive indices. Together the cornea and the lens are responsible for focussing light onto the retina. The cornea provides around two-thirds and the lens around one-third of the refractive power of the eye.
Figure 1 - Diagram Depicting Anatomy of the Eye.
12. Anterior chamber – the front part of the eye between the cornea and the iris. It is filled with aqueous humour. In general, the depth of the anterior chamber is approximately 3mm, but may be affected by age, gender, refractive error, and cataract formation.
13. Aqueous humour – an optically clear, slightly alkaline liquid that occupies the anterior and posterior chambers of the eye.
14. Choroid – the middle layer of the eye between the retina and the sclera. It provides one of the two blood supplies to the retina.
15. Ciliary body – contains the ciliary muscle which connects the choroid to the lens zonules, which are a series of fibres that hold the lens in place. The ciliary muscle is a ring of muscle, which functions to change the shape of the lens.
16. Cones – one of two types of light-receptive cells in the eye (the other being rods). Cones are active at higher light levels (photopic vision), are capable of colour vision and are responsible for high spatial acuity.
17. Conjunctiva – the mucous membrane that lines the exposed portion of the eyeball and inner surface of the eyelids.
18. Cornea – the transparent circular part of the front of the eyeball. It refracts the light entering the eye onto the lens, which then focuses it onto the retina. Both the cornea and lens refract light, and act together to focus it. Changing the shape of the cornea, or the lens therefore changes the focusing power. The cornea is comprised of the following structures, shown in Figure 2 and listed below in order of innermost structure to outermost structure:
Figure 2 - Diagram depicting structure of cornea.
i) Endothelium (a single layer of cells responsible for maintaining fluid balance);
ii) Descemet’s Membrane (a thin layer supporting the endothelium);
iii) Stroma (a thick transparent central layer);
iv) Bowman’s Membrane (a thin layer protecting the stroma); and
v) Epithelium (a thin outermost layer of fast-growing cells which easily regenerate).
19. Iris – a diaphragm structure that is able to dilate and contract to regulate the amount of light that enters the eye by changing the size of the pupil through which light enters. It forms the coloured, visible part of the eye in front of the lens.
20. Lens (crystalline lens) – a transparent structure situated behind the iris and pupil which helps to refract incoming light and focuses it onto the retina. The structure of the lens is set out in Figure 3 below:
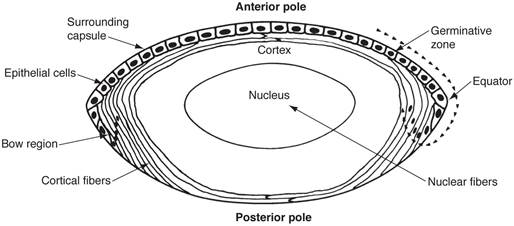
Figure 3 - Structure of the Lens.
21. The lens has a unique structure consisting of tightly packed fibre cells with a specialised organisation. The fibre cells are filled with high concentrations of water-soluble crystalline proteins which contribute to lens transparency. The lens is held in the lens capsule, which is a flat bag-like structure, the outermost side being the anterior capsule, and the innermost side being the posterior capsule (the equator of the lens capsule delineates the transition point between the anterior capsule and the posterior capsule). The lens can change shape to alter its focal length, changing the angle of light rays so that they hit the appropriate location on the retina.
22. The three layers of the lens are the nucleus, cortex, and capsule:
i) Lens capsule – the membrane completely enclosing the lens, which has anterior and posterior polarities (as shown in Figure 3).
ii) Lens cortex – the outer part of the lens which surrounds the lens nucleus and which consists of recently formed nucleated fibre cells. The fibres of the cortex are loosely arranged and as such, it has a mud-like consistency.
iii) Lens nucleus – the central structure of the lens which is made of nucleated fibre cells and is surrounded by the cortex. In contrast to the cortex, the fibres of the nucleus are closely compacted and it has a hard crystalline structure. The fibres also tend to become more compacted with increasing age.
23. Macula – a yellow spot on the retina at the back of the eye which plays a key role in visual acuity. At the centre of the macula is a small depression, called the fovea, which comprises only cones, and is particularly important for visual acuity and colour discrimination.
24. Optic disc – a small oval-shaped area on the retina marking the site of exit from the eyeball of the optic nerve. The optic disc identifies the start of the optic nerve where messages from cone and rod cells leave the eye via ganglion cells and then nerve fibres connect to the occipital cortex (seeing part) of the brain.
25. Optic nerve – a nerve which leaves the eye at the optic disc and transfers all the visual information to the brain.
26. Posterior chamber – the part of the eye between the iris and the anterior portion of the lens. It is filled with aqueous humour.
27. Pupil – the circular opening in the centre of the iris through which light passes into the lens of the eye. The iris controls dilation and constriction of the pupil.
28. Retina – a light-sensitive layer that lines the interior of the eye. It is composed of light-sensitive cells known as rods and cones.
29. Rods – one of two types of light-receptive cells in the eye (the other being cones). Rods are responsible for vision at low light levels. Rods do not mediate colour vision, and have a low spatial acuity.
30. Sclera – the dense fibrous opaque white outer coat enclosing the part of the eyeball not covered by the cornea.
31. Vitreous body – the clear colourless transparent gel that fills the vitreous chamber.
32. Vitreous chamber – the space in the eyeball between the lens and the retina that is occupied by the vitreous body.
33. Zonules – a series of fibres that connect the ciliary body to the crystalline lens and hold the lens in place. These fibres are sometimes collectively referred to as the suspensory ligaments of the lens.
The functioning of a healthy eye
34. When light enters the eye, the structure it first meets is the cornea. The cornea is transparent, so light passes through it but is refracted radially inwardly so that the light is directed through the pupil. The light then travels through the posterior chamber to the lens, which refracts the light further. This time, the lens refracts the light beams such that an image is formed on the retina. The retina’s light-sensitive cells then send impulses to the optic nerve at the back of the eye, which transmits those impulses to the brain.
35. Accommodation is the process whereby the lens geometry is changed to focus on nearer or more distant objects. To focus on a near object, the ciliary muscle contracts, allowing the zonules to loosen and the lens to therefore become rounder and thicker due to the natural elasticity of the lens. Light rays from close objects are divergent and require a stronger degree of convergent refraction to be focused onto the retina, which is enabled by the thicker lens. To focus on a distant object, the ciliary muscle relaxes, causing the lens zonules and suspensory ligaments to pull on the lens, such that the lens is pulled flat and thin, which allows a lesser refraction of the light rays. This is all that is required to focus them onto the retina, as the light rays reflected from distant objects are almost parallel when they reach the eye.
Refractive disorders
36. Short sightedness (myopia), long sightedness (hyperopia) and astigmatism are all refractive disorders resulting from an inability to focus light onto the retina. They are caused, at least in part, by curvature issues in the cornea.
37. Refractive disorders can be treated non-surgically, with glasses and contact lenses, but also surgically.
38. Radial keratotomy (RK) was a surgical procedure for the correction of myopia, whereby incisions were made in the cornea with a surgical knife in a radial pattern. The idea was that the incisions would change the shape of the cornea, altering its refractive power and enabling better focus of light onto the retina. By the priority date the RK procedure for the treatment of myopia had been superseded by laser-based techniques known as PRK, LASEK and LASIK. These are discussed further below. However, RK remained in use for treatment of astigmatism.
39. The depth of the incisions in the RK procedure were about 80-90% of the thickness of the cornea. The variability in the thickness of the cornea (it is thinner in the centre than at the periphery) required the use of a measuring technique, usually ultrasound, at the point of the incision to ensure that the cornea was not perforated. A perforation caused major clinical issues.
40. An estimated 95 million people worldwide are affected by cataracts. Cataracts remain the leading cause of blindness in middle-income and low-income countries.
41. The formation of a cataract is associated with an abnormal cross-linking of the naturally transparent proteins in the lens which may be related to age, genetic predisposition, eye trauma or other pathologies, leading generally to opacity in the lens (i.e. light scattering within the lens structure) which can affect the quality of vision. A cataract can also lead to:
i) Changes in refractive indices and therefore in focussing;
ii) Changes in geometrical shape of the lens and anterior chamber depth; and
iii) Loss of accommodation (the ability of the eye to cause changes in lens geometry and thereby change the focal point of the eye as described above).
42. The three most common types of cataract are:
i) Nuclear sclerotic cataracts, which are caused by a hardening of the lens due to compression of the nucleus and are characterized by visually significant nuclear opacity;
ii) Cortical cataracts, which occur when the part of the lens cortex surrounding the nucleus becomes opacified; and
iii) Posterior subcapsular cataracts, which are opacities located in the most posterior cortical layer, directly under the lens capsule.
43. A patient with symptomatic cataracts may report, among other symptoms, blurred or misty vision, that lights appear too bright or glaring, that they struggle to see in low light, or that colours appear faded.
44. Modern cataract surgery involves the removal of the lens material from the lens capsule and placement of an artificial intraocular lens (IOL) in the lens capsule. The aim is to both remove the opacified lens material as well as provide the patient with a good visual outcome (e.g. through choice of an IOL with appropriate refractive properties). Cataract surgery is a small-incisional surgery with rapid visual recovery, good visual outcomes, and minimal complications in most patients.
45. By 2005 a typical cataract surgery involved four principal steps:
i) Making of initial corneal incisions to access the anterior chamber (access incision);
ii) Opening of the anterior capsule (capsulotomy);
iii) Removal of the lens cortex and nucleus. This is done by aspiration (i.e. suction). The hard nucleus of the lens must be broken up first and by 2005 “phacoemulsification” (see below) was well established for this purpose; and
iv) Implantation of an IOL into the empty remaining capsule.
Initial Corneal Incision
46. An incision is typically made in the cornea (known as a ‘clear corneal incision’) although may alternatively be made in the sclera. The purpose of creating a corneal wound is to provide entry access into the anterior chamber for:
i) Viscoelastic material to be inserted to maintain the geometric stability of the eye during surgery;
ii) Instruments used to open the lens capsule and remove the lens (e.g. used for phacoemulsification); and
iii) Implantation of the IOL (IOL injection).
47. The clear corneal incision is typically a self-sealing, sutureless wound. The incision can be made radially towards the centre of the eye to support sealing and strengthen the incision.
48. A second wound called a paracentesis is typically made away from the clear corneal incision to allow insertion of a second instrument into the anterior chamber during surgery.
Anterior Capsulotomy
49. An anterior capsulotomy is a partial or fully circular cut in the anterior portion of the lens capsule with a typical diameter of between 4 and 7 mm, which is made in order to provide access to the crystalline lens within the capsule.
50. A predecessor manual method (now surpassed by Continuous Curvilinear Capsulorhexis) for achieving anterior capsulotomy is known as ‘can-opener’ capsulotomy, whereby a circular series of perforations in the anterior lens capsule (similar to those made by a can opener around the circumference of a can) are made by means of a sharp needle. A circular fragment of lens capsule is removed by tearing away the fragment along the perforations in the capsule. A disadvantage of can-opener capsulotomy is that the tears can take the form of spiked edges between adjoining perforations. These tears may extend out in a radial fashion, risking damage to the eye structures.
51. By 2005 Continuous Curvilinear Capsulorhexis (CCC) was the preferred manual method of achieving anterior capsulotomy. CCC is a manual anterior capsulotomy technique whereby a controlled circular tear is made in the anterior capsule. CCC involves a needle puncture followed by a controlled tearing of the capsule using forceps (or a needle) taken in clockwise or anticlockwise directions. The CCC method was developed in the 1980s and aimed to achieve a more circular, central cut in the anterior lens capsule, with a diameter of 4-6 mm. The advantage of CCC over can-opener capsulotomy is that, when performed correctly, the tears do not have spiked edges as the forces exerted on the capsule by the forceps are distributed. However, CCC can still result in unwanted tears or splits in the capsule towards the equator, which can lead to instability of the cataract and difficulty in removing the lens nucleus.
Lens Removal
52. Following anterior capsulotomy, the lens material (lens nucleus and lens cortex) is removed.
53. The lens capsule is first separated from the lens by a process called hydrodissection, where balanced salt solution is injected between the edge of the anterior lens capsule and the peripheral lens cortex to cleave the lens from the remaining anterior and the posterior capsule. Hydrodelineation may also be performed, where the salt solution is injected into the area between the lens nucleus and cortex. The fluid cleaves the hard, central nucleus from the cortex.
54. Following these steps, various techniques and tools can be used to remove the lens matter, dependent upon surgeon preference and the nature of the cataract to be removed. These techniques include:
i) Phacoemulsification. This technique is used to break up the lens nucleus inside the lens capsule. A “phaco probe” (a small hollow needle usually made from titanium) is inserted into the lens capsule, which vibrates longitudinally or horizontally at ultrasonic frequencies. The needle is applied to the lens nucleus, and the vibrating needle and the ultrasonic energy that it emits emulsifies the lens nucleus.
ii) Fine steel “chopper”. This is used by the surgeon to cut large pieces of the lens nucleus which are then removed by the phaco probe.
iii) Irrigation/aspiration. Irrigation and aspiration are techniques used in combination to actually effect the removal of the lens material. Fluid is irrigated into the capsule to maintain the integrity of the capsule bag, whilst at the same time the lens material is aspirated out. In the case of the lens nucleus this process of irrigation and aspiration is typically performed in conjunction with phacoemulsification and/or fragmentation techniques (due to the hardness of the nucleus). Lens cortex material (which is softer and more readily aspirated) is subsequently removed without need for phacoemulsification or fragmentation. This may be after a change to an irrigation / aspiration handpiece. Irrigation, when combined with phacoemulsification, can also provide liquid of a cooling temperature to prevent “phaco burns” from the vibrating needle.
55. These techniques can also be used in various combinations to break up and remove the lens material. Removal of the cloudy lens materials, whilst leaving the capsular bag in place, is known as extracapsular surgery.
56. Alternatively, the lens nucleus, cortex and capsule could be removed in one piece (known as intracapsular surgery). Removal of the lens nucleus and cortex in one piece generally requires a larger access incision to be made in the cornea, and therefore stiches. For this reason, since the development of extracapsular surgical techniques, the intracapsular procedure is rarely carried out.
Implantation of IOL
57. In this step, a synthetic IOL is inserted into the largely intact empty lens capsule (capsular bag), which may have been prepped for IOL insertion by injecting a viscoelastic substance into the lens capsule to prevent it from collapsing following removal of the natural lens material.
58. The portions of the lens capsule which are left intact (in particular the posterior capsule) help to stabilise the implanted IOL in the desired position and reduce post-operative complications associated with potential mispositioning of the IOL.
Figure 4 - Examples of different IOLs that can be implanted into the capsular bag
Possibility of posterior capsulotomy following cataract surgery
59. Some patients develop a thickening of the posterior capsule following cataract surgery, which results in impaired, cloudy vision - Posterior Capsular Opacification or PCO, also known as secondary cataracts. It is caused by a build-up of protein / residual epithelium cells on the posterior capsule and obscures light passing through the posterior capsule to the retina, resulting in a loss of visual acuity. PCO was a relatively common occurrence following cataract surgery, occurring in around 50% of patients within 10 years of the original surgery. It is treated by performing a capsulotomy in the posterior capsule to open up a hole through which light can pass. This capsulotomy is performed by a Nd:YAG laser (see below).
60. Although precise dimensions vary from person to person, the Skilled Team would have in mind the following dimensions as a good starting point in an adult eye: the lens is generally about 10mm in diameter and 4mm thick. The anterior capsule is about 15 µm thick and the posterior is about 5 µm. It is not entirely clear to me whether the intended diameter of an anterior capsulotomy has changed since CCC was first developed, but I note that Professor Lawless considered the diameter was generally 5-7 mm, as opposed to 4-6mm quoted above, but the difference does not matter. Finally, the distance from the epithelium (i.e. the anterior edge of the eye) to the retina is of the order of 20mm+.
Laser technology - general
61. A laser is a device that utilises the natural oscillations of atoms or molecules between energy levels for generating a beam of coherent electromagnetic radiation, usually in the ultraviolet, visible, or infrared regions of the spectrum.
62. The term ‘laser’ is generally used synonymously with laser resonators, a simple schematic of which is illustrated in Figure 5, below. At its most basic, a laser consists of three main components: a laser gain medium (which can be solid, a liquid or a gas), a stimulating energy source (pump) and an optical resonator (which in Figure 5 consists of a highly reflecting mirror and a partially reflecting mirror which acts as an output coupler). A laser gain medium is a material to which energy is applied to put atoms or molecules of the material into an excited quantum state. A photon of light, passing through the material, can stimulate the emission of a further photon from one or more of the excited atoms. This allows the amplification of an optical signal propagating through the laser gain medium.
Figure 5 - Schematic of a simple laser system.
63. Energy from the pump excites the laser gain medium which sits within the optical resonator. Light collected by the resonator circulates in a closed path (in Figure 5 this is continued reflection between the highly reflecting mirror and the output coupler), passing through the laser gain medium each time it circulates. If the laser gain medium has been sufficiently energized, emission of radiation from the laser gain medium will be stimulated by the light passing through it, amplifying the optical signal as it passes through the laser gain medium. In a steady state, amplification provided by the gain medium will equal resonator losses, and there will be a continuing feedback of energy to the light within the resonator, leading to the emission of an output beam of coherent electromagnetic radiation.
64. Lasers are characterized by a number of different parameters, including their wavelength of operation (i.e. the part of the electromagnetic spectrum in which they operate), and their temporal properties (i.e. whether they output a continuous wave, or a series of pulses and if so the duration, repetition rate and energy of those pulses). Continuous wave lasers are characterized by their average emitted power while pulsed lasers are characterized by their average emitted power, the energy of each pulse and the peak optical power of each pulse.
65. The wavelength of light (see Figure 6, below) is inversely proportional to the optical frequency and is the physical length of each oscillation within the electric field. It is parametrised in units of length. The visible part of the spectrum is generally taken to span from around 400 nanometres (nm, 10-9 m) to around 750 nm. On the longer wavelength side of the visible spectrum is a part of the spectrum referred to as ‘infrared’ and on the shorter wavelength side of the visible spectrum is a part of the spectrum referred to as ‘ultra-violet’. The wavelength at which a laser operates is dictated by the laser gain medium as well as the spectrum of the resonator, discussed further below.
Figure 6 - The electromagnetic spectrum
Laser gain media
66. The wavelength at which a laser operates is dictated in part by the laser gain medium, of which there are a very large number. A number of exemplary laser gain media are described below.
67. An ion laser is a type of gas laser where ions are used as the gain medium. The gas is held within a ceramic tube and a high electric current is used to ionise the gas and pump the laser gain medium. Gases such as argon and krypton are used. Ion lasers typically operate in the visible part of the electromagnetic spectrum, between 400 and 700 nm, but can also (depending on the specific gas mixture used) operate in the UV and infrared wavelength ranges.
68. An excimer laser has a gain medium which is a gas mixture, typically containing a noble gas (rare gas) (e.g. argon, krypton, or xenon) and a halogen (e.g. fluorine or chlorine, e.g. as HCl). The gain medium is pumped with short (nanosecond) high- voltage electric pulses, which, instead of ionising the gas, create so-called excimers (excited dimers, unstable molecules which can emit photons when disassociating). The excimers form the laser gain medium. Excimer lasers operate most commonly in the ultraviolet region of the spectrum, at wavelengths between 150 and 350 nm.
69. Solid state lasers are a broad category of lasers in which the laser gain medium is a solid, typically in the form of a crystal or glass which is doped with an ion. The wavelength of the laser is dictated by the active ion and the material in which it is doped, as well as the resonator. Solid state lasers are typically optically pumped (optical energy is used to stimulate the laser gain medium) using flash lamps, arc lamps, semiconductor lasers, or other solid-state lasers. Solid-state lasers typically operate in the infrared region of the electromagnetic spectrum, between 700 and 3000 nm (3 μm). Solid-state lasers include Nd:YAG, Ho:YAG and Er:YAG lasers. These employ a yttrium aluminium garnet crystal that has been doped with rare earth ions such as neodymium Nd, holmium Ho or erbium Er ions as a laser gain medium. Nd:YAG lasers typically operate at 1064 nm. Another solid state laser is Ti:Al2O3 (or Ti:Sapphire) which employs sapphire (a variety of corundum) doped with titanium ions as the laser gain medium. This laser is notable because the laser gain medium can operate across a relatively broad spectral range, meaning that (depending on the properties of the optical cavity) such lasers can be made to operate at wavelengths between about 700 nm and 900 nm. The broad bandwidth can also support the generation of ultrashort pulses (see further below). Further examples of solid state lasers include fibre lasers, which employ lengths of glass optical fibre doped with rare earth ions such as ytterbium or erbium as laser gain media, operating around 1064 nm or 1550 nm, respectively.
Continuous wave and pulsed laser operation
70. Lasers are broadly separated between continuous wave and pulsed lasers. A laser is said to be ‘continuous wave’ (or CW) when it emits radiation at a relatively constant optical power. Lasers can, through a number of different techniques, be made to deliver optical pulses - the optical power is not constant in time but instead the power is delivered as a series of discrete pulses separated in time. Figure 7, below, shows the profiles of CW laser emission (left) vs pulsed laser emission.
Figure 7 - CW laser emission (left) vs pulsed laser emission (right)
71. The most important temporal parameters defining the output of a pulsed laser are the duration of the pulses (also referred to as pulse width), the repetition rate (i.e. the number of pulses per unit time), the optical power or optical energy of the pulse, and the averaged power of the pulse train. For a pulsed laser, the optical power varies with time, and both the peak power (i.e. the maximum instantaneous optical power) and the average power may be referred to. The pulse energy is the total amount of energy delivered by each optical pulse and will be given by the integral over time of the optical power of one pulse (i.e. the area under one pulse as shown in Figure 8).
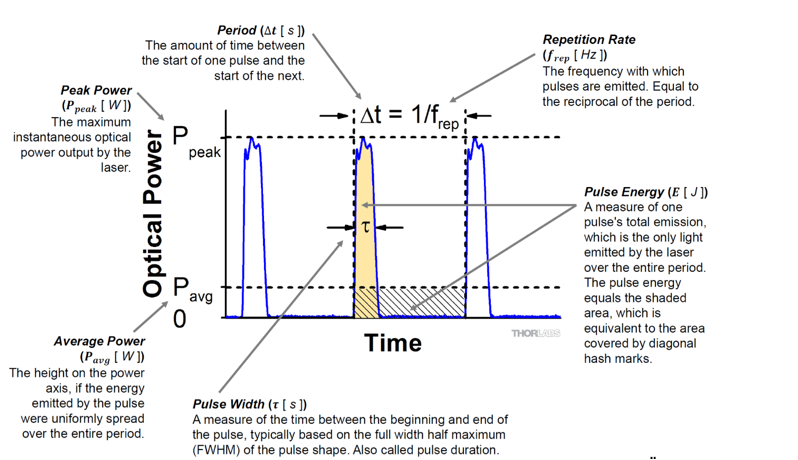
Figure 8 - Key parameters of pulsed laser output
72. The pulse duration and repetition rate are dependent upon a number of factors in the laser gain medium, the optical resonator, and particular techniques which are used to provide lasers with particular temporal properties. The pulse duration is parameterised in units of time and can range from durations on the order of seconds down to the order of femtoseconds. For completeness, the unit prefixes used are as follows:
Millisecond (ms) 10-3 s Microsecond (μs) 10-6 s Nanosecond (ns) 10-9 s Picosecond (ps) 10-12 s Femtosecond (fs) 10-15 s
73. A number of exemplary methods of pulsed laser operation are described below.
74. Pulsed laser operation can arise from the use of a pulsed pump source. For example, excimer lasers typically provide pulses on the order of a few nanoseconds, but sometimes longer, of the order of 100 ns, with repetition rates as low as 10 Hz but can reach up to 1 kHz. This largely reflects the pulse duration and repetition rate of the electrical pulses which are used to pump the laser gain medium.
75. Another mechanism which is used to provide pulsed laser output is Q-Switching. In this method an ‘Q-switch’ (typically an optical modulator) is provided within the optical resonator, which controls the total loss within the optical resonator. This is used to hold the overall losses within the resonator above the threshold for laser operation. During this time, the laser gain medium continues to be pumped, increasing the amount of energy stored. The loss imparted by the Q-switch is then reduced, such that the loss within the resonator is reduced below the threshold for feedback within the resonator to lead to the rapid accumulation of energy within the resonator. Q-switching creates pulses whose duration is on the order of a number of ‘round trip’ times within the resonator (i.e. the time taken for the light to pass from one end of the resonator to another, accumulating energy from the laser gain medium through each pass). Typically, such systems create pulses with a duration on the order of 10s - 100s of nanoseconds. These systems can be used to generate single pulses, or the modulation of the loss within the resonator can be at regular intervals to produce a train of pulses on the order of 10s of kHz. This technique is often employed with solid-state lasers such as Nd:YAG lasers.
76. Another mechanism which is used to provide pulsed laser output is mode-locking. The laser resonator contains a mode locking device, either an active element (such as an optic modulator) or a nonlinear passive element (such as a saturable absorber). In a typical (continuous wave) laser resonator, there are a number of different longitudinal modes which, effectively, act as independent lasers operating at discrete, closely spaced wavelengths. The effect of the mode locking element is to force a fixed phase relationship to all of the longitudinal modes of optical radiation within the resonator, resulting in a constructive interference effect which causes the circulating laser light to take the form of a laser pulse circulating within the resonator at the round-trip time of the resonator. The output of the laser is then in the form of a train of pulses, whose repetition rate is determined by the round-trip time of the resonator. The duration of the pulse is determined by the number of different modes resonating in the resonator, which is determined by the resonator itself and also the bandwidth of the laser gain medium (i.e. the range of wavelengths across which the laser gain medium can support laser operation). This technique can allow for the generation of pulses with durations on the order of a few 10s of picoseconds down to 100s or even 10s of femtoseconds. Optical pulses of this duration are typically referred to as ‘ultrashort’ pulses. Solid-state mode-locked lasers are the dominant type of mode-locked lasers.
Gaussian beam optics
77. In optics and particularly in laser physics, laser beams often occur in the form of Gaussian beams, which are defined as beams in which the transverse profile of the optical intensity of the beam can be described with a Gaussian function.
78. Laser beams cannot be focussed to an infinitesimal point, but instead, due to diffraction, a Gaussian beam will converge and diverge from an area called the beam waist (w0), which is where the beam diameter reaches a minimum value. This is illustrated in Figure 9, below:
Figure 9 - Beam waist (w0) of a Gaussian beams
79. Also illustrated in Figure 9 is the divergence angle θ. A small beam waist results in a larger divergence angle, while a large beam waist results in a smaller divergence angle (or a more collimated beam). Another important parameter of the beam is the Rayleigh range, defined as the distance (z) from the beam waist where the cross-sectional area of the beam is doubled, or equivalently where the width of the beam has increased to √2 w0. The Rayleigh range (zR) can be expressed as: where
where  is the wavelength.
is the wavelength.
Lenses
80. Optical lenses are components which refract rays of a light beam directed there through, so as to converge (focus) or diverge the beam. A simple lens is formed from a single piece of material shaped to provide the desired refraction of light, whereas a compound lens consists of several simple elements arranged in series, usually along a common optical axis.
Figure 10 - Focal points and focal lengths for divergent (left) and convergent
(right) lenses
81. Lenses each have a focal point (F). The distance between the focal point (F) and the centre of the lens is the focal length (f). For a converging lens, the focal point is the point through which the light rays which are initially parallel to the principal axis (the axis which runs through the centre of the lens) pass, after they have been refracted by the lens. The focal point of a diverging lens is the point from which light rays which are parallel to the principal axis prior to refraction appear to have come from after refraction by the lens.
82. The focussing properties of a lens are defined by the refractive indices of the media through which light passes (e.g. the lens material and air) and the angle of incidence at the interface between the media. For a lens in air, the focal length of a lens can be calculated using the lensmaker's equation:

where f is the focal length of the lens, n is the refractive index of the lens material, R1 is the radius of curvature of the lens surface closer to the light source, R2 is the radius of curvature of the lens surface farther from the light source, and d is the thickness of the lens.
83. Aberrations refer to the distortion in an image formed by a lens. Lens systems may be designed to minimise aberrations for a specific application. Conversely, lens systems may be designed so as to intentionally introduce aberrations.
84. Surfaces of lenses are often formed as spherical surfaces, for ease of manufacturing. However, a spherical surface causes light rays which are parallel to, but radially distant from, the principal axis to be focused with a different focal length than the rays which are radially close to the axis. As not all of the rays are focused to a single, sharp point, the resulting image is blurred.
85. When rays are focused to differing focal points due to cylindrical imperfection in the formation of components in the optical system (e.g. formation of a lens surface which is not spherical, but has some cylindrical aspect), the aberration is referred to as “astigmatism”.
86. Chromatic aberration occurs when a lens focusses different colours to different points, and occurs because the refractive index of the material varies with wavelength of incident light (dispersion).
87. An achromatic lens or achromat is a lens that is designed to limit the effects of chromatic and spherical aberration. Achromatic lenses are corrected to bring different wavelengths into focus. The most common type of achromat is the achromatic doublet, which is composed of two individual lenses made from glasses with different dispersion characteristics.
Galvanometric mirrors
88. A Galvanometer is an instrument for measuring small electrical currents by deflection of a moving coil. When current flows, the coil experiences a proportional torque.
89. In galvanometric scanners (also referred to as “galvanometric mirrors” or “galvos”), a mirror is coupled to the coil, such that it can be manipulated by the galvanometer. Currents can be driven through the galvanometer to induce fine and fast movement of the mirror, often with a servo-like control loop.
90. In optical systems, galvanometric scanners can be used to scan a light beam in the transverse plane. F-theta lenses are designed to focus a laser beam onto a planar image plane. They are often used in a scanning system with two galvanometer mirrors. One mirror is responsible for beam deflection in one direction and the second one for the perpendicular direction.
Beam splitters / Beam combiners
91. A beam splitter is a partially reflective optical device for splitting an incident beam of light into a plurality of separate beams. Used in reverse, beam splitters can also be used to combine a plurality of incident beams into a single beam. When used to combine beams, the devices are also referred to as “beam combiners”.
92. Generally, a beam splitter splits the incident beam such that a portion of the light is transmitted through the beam splitting device, and the rest is reflected. In practice, some of the incident light will be absorbed or scattered by the beam splitter. The properties of the beam splitter can be selected such that, for a certain wavelength of light, a specific proportion of the light is reflected.
93. Polarising beam splitters can be used to split light into beams of differing polarisation states (the orientation of the oscillations of electric field component of the light wave, with respect to the direction of motion of that wave). For unpolarised light, a polarising beam splitter can be used to split the light evenly into reflected and transmitted beams having differing polarisations. Non-polarising beam splitters split the incident beam into beams without altering the polarisation state.
94. A “half-silvered mirror” refers to a substrate having a partially transparent coating of silver. The thickness of the metal coating determines the proportion of the incident light which is transmitted there through, and the proportion which is reflected. Partially reflecting / transmitting mirrors are also commonly made by depositing layers of transparent materials having alternating high and low indices of refraction. To provide spectrally selective beam splitting, a dichroic material can be used as the coating. Depending on the characteristics of the dichroic coating, the ratio of light reflected to that transmitted will vary as a function of the wavelength of the incident light. Beams splitters employing dichroic coatings are also referred to as “dichroic mirrors”.
Laser-tissue interaction
95. Lasers can interact with tissue of the human body in a number of ways. Surgical lasers employ properties of the laser light to effect a destructive interaction with the tissue. The mechanism by which the interaction occurs is dependent upon the properties of the laser light, including its wavelength, its average power, and (if it is pulsed) the pulse energy and pulse duration (peak power) as well as the illuminated area defining the pulse intensity or irradiance [Units: W/cm2].
Photochemical interaction
96. Photochemical interaction, sometimes referred to as photoactivation, can take place at long exposure times, ranging from seconds to continuously, and relatively low power densities or irradiances (typically 1 W/cm2). This type of interaction is based on the use of a photosensitizing dye (e.g., rose bengal, riboflavin, or verteporfin), which serves as a chemical (electron reaction) catalyst. Laser irradiation, at a wavelength coupled to the specific dye used, causes a photochemical reaction only within tissues where the dye is present and when irradiated. The dye used therefore dictates the wavelength and hence type of laser used.
Photothermal interaction
97. Photothermal interaction refers to a broad class of interactions of laser light with tissue typically in which laser light with a relatively high power density is used to locally raise the temperature of the tissue leading to destruction of the tissue. Similarly, photothermal effects can occur even with low power densities but high absorbances and long duration exposure. Typically, power densities of 10 W/cm2 to 106 W/cm2 and pulse durations on the order of μs to seconds might be used. The thermal interactions induced by the laser energy includes coagulation (denaturation of proteins and collagen) for temperatures above 60°C, and vaporization above 100°C. Natural chromophores in the tissue may absorb the laser light, leading to the local heating. The tissue type, and absorption bands of the natural chromophores therein, dictate the type of laser used, which should be matched to the chromophore.
98. The main natural chromophores within ocular tissues that are targeted during photocoagulation are haemoglobin (e.g., in blood vessels) and melanin (e.g., in the iris or deep retinal layers), which strongly absorb wavelengths from about 400 nm to 580 nm. High power lasers operating in the visible wavelength range, such as argon ion lasers or frequency doubled Nd:YAG lasers are typically used to this end.
Photoablation
99. In photoablation, the laser energy is highly absorbed in a thin surface layer of tissue. This results in ejection of fragments and very clean ablation with clinically insignificant necrosis or thermal damage to adjacent tissue. The target tissue components are ablated without generation of any considerable damage at the edges. Typical threshold values for this type of interaction are irradiances of 107 to 108 W/cm2 and pulses in the nanosecond range.
Photodisruption
100. In further contrast to both photochemical/photothermal interactions, and to photoablation, photodisruption exploits the local ionisation (disassociation of electrons from atoms) of tissue, leading to the formation of a plasma which in turn rapidly expands as a bubble of plasma (a gas made up of charged particles). Within a liquid environment, such as within a tissue, the plasma expansion leads to disruption of the local tissue. This requires the use of ultrashort pulses (i.e. a few picoseconds or 10s to 100s of femtoseconds) with a high peak intensity (peak power per illuminated area). The mechanism of photodisruption relies on a high intensity optical field causing the dissociation of electrons from their atoms and then accelerating them. This in turn leads to the local ionisation of the tissue and the formation of a bubble of plasma, which expands and collapses. The cavitation of the plasma bubble leads to the formation of an acoustic shock wave. Expansion, collapse and shock waves can disrupt the tissue.
101. Because the process relies on a high peak intensity (typically at the focus of the laser beam), photodisruption can be achieved using a laser wavelength to which the tissue is transparent at low light intensities. The photodisruption will occur only where the local intensity exceeds a threshold intensity for dielectric breakdown of the tissue.
102. Photodisruption requires the use of q-switched (nanosecond) or ultrashort pulses because, as per the definition of intensity (energy per unit time per area), for a given pulse energy per area, a short duration pulse will have a peak intensity that will be very high. To further increase the intensity, the beam can be focussed because the peak intensity is a function not only of the peak pulse power, but also the size of the beam waist. A smaller beam waist gives rise to greater local intensity at the beam waist for a given pulse energy.
103. This is shown schematically in Figure 11 below, which is a diagram of two laser pulses, the orange pulse representing a pulse which is of a shorter duration (in time), or has a narrower beam width (in space) than the blue pulse. The total energy of the two pulses (represented by the area under each curve) is the same. As shown, for a given pulse energy, reducing the duration of the beam or the width of the beam increases the peak instantaneous local intensity, such that it is able to cross a given threshold for photodisruption in tissue.
Figure 11 - Laser pulse schematic diagram.
Femtosecond Lasers
104. A femtosecond laser is an ultrashort pulsed laser, in which the power of the laser is delivered via a series of optical pulses. The duration of each pulse is in the order of femtoseconds (10-15 s).
105. Femtosecond lasers, as well as nanosecond and picosecond lasers, were capable of producing photodisruption.
106. The shorter the laser pulse, the more controlled and precise the photodisruption. That is because the size of the plasma bubble is related to the amount of energy input to exceed the threshold intensity required for photodisruption to occur. A smaller bubble of plasma created at the focal point of the laser generates a smaller cavitation bubble and smaller shockwaves which localises the effect of the laser and reduces collateral effects on adjacent tissue.
107. Whilst there are a number of factors at play (see above), in general, a femtosecond laser will produce photodisruption at a lower threshold energy than a picosecond or nanosecond laser and will accordingly produce a smaller plasma bubble, as follows:
|
Laser pulse duration |
Plasma bubble diameter |
|
Nanosecond |
100s of microns |
|
Picosecond |
50 - 100 microns |
|
Femtosecond |
~ 10 microns |
Use of Lasers in Ophthalmology
108. PCO: Historically PCO was treated by opening up the eye and using a surgical blade to create an opening in the posterior capsule. The blade entered from an angle behind the lens. By the Priority Date, a Nd:YAG laser was used instead to open the posterior capsule by photodisruption.
109. Alternatives to phacoemulsification: At the Priority Date two alternatives to phacoemulsification for fragmentation of the lens in cataract surgery were known, although it was also known that these were slow and struggled to deal with dense cataracts. These were:
i) Dodick Laser Photolysis: An Nd:YAG laser was fired at a titanium plate in the handpiece, creating high intensity ultrasonic shock waves to break up lens tissue.
ii) Er:YAG laser (Asclepion-Meditec Phacolase MCL-29): An Er:YAG laser was focussed directly into the lens nucleus using a fibre optic guide. Unlike Nd:YAG lasers, which relied upon photodisruption, the Er:YAG laser relied upon a photoablative effect.
110. Refractive disorders: Historically, surgery involved use of a surgical knife to make incisions in the cornea to affect its shape and refractive properties. However, by the Priority Date different procedures were carried out using lasers:
i) Photorefractive keratectomy (“PRK”): The epithelial layer of cells covering the outside of the cornea is removed using mechanical means (a blade, scraper or specialised brush) and an excimer laser used to photoablate two layers of the cornea - Bowman’s layer and the stroma.
ii) LASIK: Instead of removing the epithelial layer of cells, a hinged flap is cut using a surgical blade (called a microkeratome) to provide direct access to the stroma. The excimer laser is then used to photoablate the stroma. Due to the cutting of the flap, photoablation of Bowman’s layer is unnecessary. The flap is self-sealing.
iii) LASEK: The epithelium is moved to one side using an alcohol solution and a thin sheet to provide access to the stroma. Once photoablation with the excimer laser is complete, the epithelium is moved back into place.
111. Glaucoma and retinal complaints: Nd:YAG lasers with nanosecond pulses were used to perform various procedures including goniopuncture, peripheral iridotomy, cutting of pupillary members, selective laser trabeculoplasty (SLT) and endoscopic vitreoretinal surgery.
112. Outlined below are a number of imaging techniques that can be employed for the imaging of the eye. Generally speaking, such imaging involves four major steps:
i) Backscattering of energy from the substructures of the eye.
ii) Detecting the backscattered / backreflected energy by means of detectors to generate a detector signal.
iii) Image / signal correction by taking into account the wave propagation or imaging errors of the detection path.
iv) Processing of the corrected image / signal to derive parameter measurements (e.g. thickness of cornea, anterior chamber depth, lens thickness) and/or generate a visual image of the measured substructures of the eye.
Confocal microscopy
113. Confocal microscopy is a microscopic imaging technique that uses a spatial pinhole to eliminate out-of-focus signals that are reflected from a sample. Volumetric images are built up by scanning the focal point of a laser beam through a sample, collecting the backscattered radiation, and spatially filtering the returning radiation by imaging it onto a pinhole so that only the light from the focal point is detected, and not light scattered from the surrounding parts of the sample.
Figure 12 - Schematic of a confocal microscope
114. A confocal scanning microscope as shown schematically in Figure 12 essentially works as follows. Light (e.g. a laser beam) is tightly focused onto the sample, using a microscope objective, so that only a small point within the sample is illuminated.
115. Light coming back from the focus point (e.g. through scattering in the sample, or fluorescence light induced in the sample) is imaged to a small pinhole and transmitted to a photodetector.
116. Light coming from other longitudinal or transverse positions in the sample is largely suppressed by the pinhole. At other lateral positions, there is hardly any incident light, except somewhat before and after the beam focus due to the substantial beam divergence. Also, such light could not get through the pinhole, since it would be focused to points away from the hole.
117. Light from positions in the sample above or below the beam focus are also suppressed by the pinhole, because the focus position of such light is not in the plane of the pinhole.
118. In this way, the intensity of the signal recorded at the detector ideally conveys information on just the single object point within the sample to which the incident light is focussed.
119. A complete two-dimensional or three-dimensional image is obtained by systematically translating the beam focus (with some kind of beam scanner, e.g. with oscillating mirrors) within the sample. The intensity from different points is recorded and is proportional to the light scattered or emitted from each of those points. In this way, an image of the sample in a particular plane or within a particular volume is built up by scanning across points in that plane or volume.
Optical coherence tomography (OCT)
120. OCT performs high-resolution, cross-sectional imaging by measuring backscattered or backreflected light, based on the interference of a light beam with a coherent replica of itself.
121. There are, broadly, two types of OCT - time domain OCT and Fourier domain OCT. Imaging devices using both were known by the Priority Date. Time-domain OCT was developed first (around 1985-1995) and Fourier-domain followed (around 1996-2000). Fourier-domain had a faster scanning time than time-domain.
122. Time domain OCT exploits the principle of temporal coherence in optical signals. At a high level, a light beam is said to have a high degree of coherence if spatially separated parts of its optical field can, when combined, interact with each other to produce constructive and destructive interference. Conversely, for an optical field with a low degree of coherence, constructive or destructive interference will only be observed between very closely spaced parts of the optical field. This is often parameterised in terms of the ‘coherence length’ of an optical field. If a light beam is split into two parts (e.g., by a beam splitter) and recombined again after one part of the light beam is spatially / temporally shifted with respect to the other part of the beam, interference between the two beams can only be observed if the shift is within the coherence length.
123. For a given light source there is an inverse relationship between optical bandwidth (i.e., the width of the optical spectrum) and the coherence length – a narrow bandwidth light source will exhibit a very long coherence length, whilst a broad band light source will exhibit a short coherence length.
124. Detection of the back scattered or backreflected light is achieved by using an optical interferometer (Michelson Interferometer). The fact that light will only exhibit interference when path lengths are matched to within the interference length is used in OCT to obtain depth range information from a scattering medium. This is achieved by splitting the light of a low-coherence light source (e.g., super-luminescent diode, broad band laser) into two different optical pathways - a reference arm and a sample arm – by means of a beam splitter. The focal point of the sample arm may be adjusted by the x-y scanners and in the z-direction by the moving lens component. The eye is placed within the sample arm. The light interference signal is detected. By processing that signal, taking into account the refractive index of the eye structures and compensating for any field distortion / aberrations of the scanning device, an image can be produced and geometrical dimensions of the eye can be derived.
125. A schematic representation of time domain OCT is shown in Figure 13, below:
Figure 13 - Time domain OCT
126. In time domain OCT the optical path length of the reference arm is swept in time, typically by periodically moving a mirror placed in the reference arm. The signal at the detector is recorded as the mirror is swept along a series of positions (z). As the mirror is swept, it will move into positions where the optical path length of the reference arm is matched (within the coherence length of the light source) to the optical path length in the sample arm of scattering surfaces in the sample. As shown in the graph in the bottom left corner of Figure 13, at these positions interference fringes will be seen in the detector signal as the light from the reference and sample arms constructively and destructively interferes. The amplitude of this signal, as a function of depth z within the sample, will be proportional to the strength of scattering at that depth. This signal is demodulated, and the demodulated signal shows peaks corresponding to the positions at which the path length of the reference arm was matched to the path length to scattering surfaces in the sample, the intensity of those peaks is proportional to the strength of scattering from those surfaces.
127. To build up a volumetric image, the beam is scanned in the x-y direction. For each x-y point within the sample, an axial scan (a-scan) is recorded, to record information on the location of scattering surfaces at that x-y point. By scanning across the sample and taking a-scans at a number of points, a volumetric image of the sample (in x-y-z space) can be built up.
128. A schematic representation of one type of Fourier domain OCT system is shown in Figure 14, below. This type is commonly referred to as spectral domain OCT.
Figure 14 - Fourier domain OCT
129. Fourier domain OCT exploits the fact that for an optical field interfering with itself (i.e. in the recombined beam), there is a mathematical relationship (Fourier transformation) between the interference pattern recorded as a function of temporal displacement and the spectral power density (i.e. the relative intensity of different wavelengths of light in the recombined beam).
130. In Fourier domain OCT, the path length in the reference arm is fixed and the optical spectrum of the recombined light is recorded, for example using a spectrometer. Interference between light from the sample and reference arms results in a modulation of the optical spectrum that is recorded - the optical spectrum will exhibit a series of peaks and troughs which arise from the interference of different wavelengths of light in the light from the reference and sample arms. The shape of the spectrum will be a function of the structure of the scattering surfaces in the sample arm. A mathematical function known as a Fourier transform is applied to the spectrum and this will provide a signal as a function of depth z within the sample proportional to the strength of scattering at that depth.
131. As with time domain OCT, the sample arm is scanned in the x-y direction through the sample, with an axial scan taken at various positions, so as to build up a volumetric image of the sample. There were two ways to gather depth information. The first way was to move the mirror in the reference arm. This scans the ‘coherence gate’ of the OCT system through the depth of the tissue. The second way was to sweep the mirror in the reference arm and simultaneously sweep the depth of focus of the sample beam within the tissue. This was sometimes referred to as Optical Coherence Microscopy (OCM) and was a well-known configuration of OCT in 2005. This is achieved typically by using a higher numerical aperture focusing optic with the sample beam, enabling better axial resolution than relying on the ‘coherence gate’.
Confocal Microscopy and OCT in context
132. In the context of medical imaging, two important characteristics of a given imaging technique are the penetration depth of the imaging technique (that is, how far into a given tissue the imaging system can detect back reflected light) and the resolution of the imaging technique (that is, what is the size of the smallest structure that can be resolved by the imaging system). For both confocal microscopy and OCT, the axial and transverse resolutions are typically not the same.
133. Commercial OCT devices for ophthalmological applications were known by the Priority Date:
i) OCT devices were used in cataract surgery for measuring the distances between the cornea, lens and retina. These included the Zeiss “IOL Master”;
ii) OCT devices which produced detailed images of the posterior segment of the eye were the standard of care for the diagnosis and treatment of glaucoma and macular disease;
iii) Axial resolution was approaching the single-digit micron range (i.e. less than 10 microns) and lateral resolutions of a few 10s of microns.
134. In his first report, Professor Bouma was content to adopt the figure shown below (taken from a current website) as representing the penetration depth and resolution of OCT. This figure was presented without explanation but it is clearly concerned with turbid tissue (i.e. not this case). This figure plainly did not represent the penetration depth of OCT in the ophthalmic context, either at the priority date or today:
135. The basic principles of fluorescence (including multiphoton fluorescence) were known:
i) Fluorescence is the emission of light after absorption of one or more photons;
ii) In multiphoton fluorescence two (or more) photons whose sum energy satisfies the energy required for excitation simultaneously arrive at the sample and are absorbed;
iii) The wavelengths of light which are absorbed and emitted by a sample are dependent upon the arrangement of the energy levels of the atoms of that sample. The wavelengths of the light which is absorbed and that which is subsequently emitted can be indicative of the make-up of the sample.
136. Professor Mrochen gave unchallenged evidence that, although the principle of multiphoton fluorescence (MPF) was known to the SE by 2005, it was not a technique used in ophthalmology and there were no commercial devices available for ophthalmic use that employed it. It had a niche use for histology or investigation of biological processes in cells at very high resolution, but with a limited imaging region.
137. All of the above was CGK. There remained, however, significant disputes over further aspects of the CGK. I return to consider these after I have considered the Patents and identified the attributes of the Skilled Team.
138. What I have set out above is more than enough technical background to understand the Patents. I will deal with the Patents at this point because this is a case in which the Patents provide an important and relatively clear indication as to the skills and knowledge of the Skilled Team (cf. Pumfrey J. in Horne Engineering at [14], which I cite below).
139. The parties only found it necessary to address the specification of EP861 and I will do the same. A key dispute between the parties concerns how to characterise the inventive concept in each Patent. Alcon submitted that the Patents describe the inventions at a very high level of generality; that very little is given in terms of technical detail; that the Patents assume the skilled team is capable of tackling the real work of actual implementation; that the Patents contain no teaching as to how the claimed systems actually perform in practice and no real data regarding performance.
140. For its part, AMO submitted that, in addition to describing the systems claimed, including a number of suitable variants, the Patents contain much practical information about how the system(s) can be used to carry out the claimed procedures. I will endeavour to highlight the practical information on which AMO relies and assess it, but this forms part of my assessment of what the Patents assume as the CGK of the Skilled Team. For the purposes of that assessment I focus in particular on the following three key areas:
i) The characteristics of the laser.
ii) The capability of the imaging system.
iii) The capability of the control system.
141. The field of the invention is identified in [0001]. The invention is said to relate to “ophthalmic surgical systems”.
142. The Background section identifies cataract surgery as being one of the most common procedures in the world, with millions of patients undergoing the procedure each year. The steps of anterior capsulotomy (both can-opener and CCC) and fragmentation of the lens (phacoemulsification) are discussed and problems with both identified.
143. At [0004] a number of problems with anterior capsulotomy, even using the CCC procedure, are noted related to the inability of the surgeon “to tear a smooth circular opening of the appropriate size without radial rips and extensions”.
144. Similarly, at [0005], it is said of phacoemulsification that: “These are the longest and thought to be the most dangerous step in the procedure due to the use of pulses of ultrasound that may lead to inadvertent ruptures of the posterior lens capsule, posterior dislocation of lens fragments, and potential damage anteriorly to the corneal endothelium and /or iris and other delicate intraocular structures…A variety of surgical maneuvers employing ultrasonic fragmentation and also requiring considerable technical dexterity on the part of the surgeon have evolved…These are all subject to the usual complications associated with delicate intraocular maneuvers (Gimbel, Chapter 15: Principles of Nuclear PhacoEmulsification, in Cataract Surgery Techniques Complications and Management 2nd Ed. Edited by Steinert et al, 2004, 153-181, incorporated herein by reference).”
145. In [0006], the Patent describes PCO (estimated to occur following cataract surgery in approximately 28-50% of patients, with Steinert Ch.44 given as the source) and identifies it as one of the principal sources of visual morbidity following cataract surgery. It states that the problem is thought to occur due to residual epithelial cells left in place near the equator of the lens. Surgical dissection is cited as an initial technique to solve the problem with ‘more recently’ the use of a Nd:YAG laser to make openings centrally in a non-invasive fashion.
146. [0006] goes on to state that most of these techniques can be considered relatively primitive requiring a high degree of manual dexterity on the part of the surgeon and the creation of a series of high energy pulses in the range of 1 to 10mJ manually marked out on the posterior lens capsule, taking great pains to avoid damage to the intraocular lens. The coarse nature of the resulting opening is said to be illustrated in Fig 44-10 in Steinert, Ch. 44.
147. [0007] acknowledges two prior art patents including that ‘Use of optical tomography in surgical procedures is described in EP 0 697 611.’
148. At [0008], the patentee sets out the problem that it intends to solve, namely “ophthalmic methods, techniques and apparatus to advance the standard of care of cataract and other ophthalmic pathologies”.
149. The Summary of the Invention section identifies the patentee’s solution to the problem, namely that the techniques and system disclosed enable “rapid and precise openings in the lens capsule and fragmentation of the lens nucleus and cortex” by use of “3-dimensional patterned laser cutting” [0009]. Various promises are made, including reduction of the duration of the procedure; reduction of the risk associated with anterior capsulotomy and fragmentation; and increased precision [0009].
150. From [0015] onwards, the Detailed Description of the Preferred Embodiments describes a system that can project/scan an optical beam into a patient’s eye by reference to Fig. 1: the optical beam is a laser, controlled by control electronics.
151. In [0016], the Patent suggests using a surgical laser configured to provide one or more of the following parameters:
i) Pulse energy up to 1 µJ, repetition rate up to 1 MHz, pulse duration ˂ 1 ps.
ii) Pulse energy up to 10 µJ, rate up to 100 kHz, pulse duration ˂ 1 ps.
iii) Pulse energy up to 1000 µJ, rate up to 1 kHz, pulse duration ˂ 3 ps.
[0016] goes on to suggest using wavelengths in the near-infrared range: 800-1100nm, because tissue absorption and scattering is reduced. The final combination of parameters suggested is low energy ultrashort pulses of near-infrared, with pulse durations below 10ps or below 1ps alone or in combination with pulse energy not exceeding 100 µJ at high repetition rate including rates above 1 kHz and above 10 kHz.
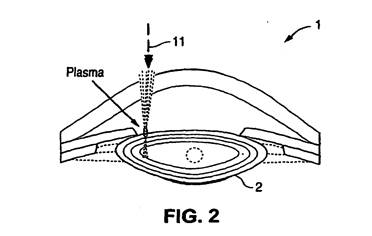
152. By reference to Fig.2 (shown below) [0017] explains photodisruption and provides an equation for calculating the laser focal spot diameter for a given wavelength of light and focussing element. It gives a worked example leading to a focal spot diameter of 15 µm. Although none of the experts gave specific evidence to this effect, I consider the Skilled Team reading the Patents would understand the significance of this figure - it is the thickness of the anterior capsule in a typical adult eye.
153. [0018] assumes the rupture zone R = 15 µm. For an AC 8mm in diameter D, the required number of pulses is N = πD/R = 1675. The Patent goes on to explain that for smaller diameters, the number of pulses would be less and the same for a larger rupture zone.
154. [0019] explains that to produce an accurate circular cut, the pulses should be delivered over a short eye fixation time i.e. more quickly than the eye moves. It assumes a fixation time t = 0.2s which would require a laser repetition rate of 8.4 kHz.
155. [0020] continues the analysis for a focal spot diameter of 15 µm. Based on certain assumptions which are set out, an estimate of the diameter of the cavitation bubble created by 4ns pulses is provided - 48 µm. Having given that estimate, [0021] then says that the energy level can be adjusted to avoid damage to the corneal endothelium. The expert evidence did not assist in explaining why damage to the corneal endothelium would be a real concern when performing an anterior capsulotomy, where the anterior capsule is some distance (probably at least 4mm) from the corneal endothelium. Be that as it may, [0021] goes on to provide various suggestions for reducing the energy level - by reducing the pulse duration (0.1 - 1ps) or reducing the pulse energy (e.g., down to 7 and 9 µJ). It explains:
‘These are only two examples, Other pulse energy duration times, focal spot sizes and threshold energy levels are possible.’
156. [0022] discusses further possible variations, in repetition rate and pulse energy to provide a focal spot diameter of 4 µm.
157. To summarise this section therefore, the Patent suggests that the laser be a pulsed surgical laser with a pulse duration in the picosecond range. The Patents do contemplate pulse durations in the high femtosecond range (e.g. perhaps 500fs) but the Skilled Team would be struck by the absence of explicit mention of femtosecond lasers. Then the Patent explains photodisruption; the basic maths required to ensure continuous cutting of tissue using a series of pulses; the relationship between threshold energy and bubble diameter; the relationship between pulse duration and energy level (i.e. picosecond pulses have higher energy levels than femtosecond pulses); and the fact that a high repetition rate and low pulse energy can be used for tighter focussing of the laser beam. Alcon submitted that all of this information, essentially about the available characteristics of the laser, would be part of the CGK and I agree.
158. In [0023] the specification turns to imaging:
‘The laser 10 and controller 12 can be set to locate the surface of the capsule and ensure that the beam will be focused on the lens capsule at all points of the desired opening. Imaging modalities and techniques described herein, such as for example, Optical Coherence Tomography (OCT) or ultrasound, may be used to determine the location and measure the thickness of the lens and lens capsule to provide greater precision to the laser focusing methods, including 2D and 3D patterning. Laser focusing may also be accomplished using one or more methods including direct observation of an aiming beam, Optical Coherence Tomography (OCT), ultra-sound, or other known ophthalmic or medical imaging modalities and combinations thereof.’
159. [0024] and Fig. 4 describe use of OCT imaging to identify the axial location of the anterior and posterior lens capsules, boundaries of cataract nucleus and depth of anterior chamber. It is said that this information may be used to program and control the subsequent laser procedure. This point is picked up again at [0026] which returns to Fig 2 and says:
Fig.2 illustrates an exemplary illustration of the delineation available using the techniques described herein to anatomically define the lens. As can be seen in Fig.2, the capsule boundaries and thickness, the cortex, epinucleus and nucleus are determinable. It is believed that OCT imaging may be used to define the boundaries of the nucleus, cortex, and other structures in the lens including, for example, the thickness of the lens capsule including all or a portion of the anterior or posterior capsule. In the most general sense, one aspect of the present invention is the use of ocular imaging data obtained as described herein as an input into a laser scanning and/or pattern treatment algorithm or technique that is used as a guide in the application of laser energy in novel laser assisted ophthalmic procedures. In fact, the imaging and treatment can be performed using the same laser and the same scanner. …’ (my emphasis)
160. In other words, an imaging device, such as an OCT device, is used to create an image of the lens which is used to control where the laser fires into the eye.
161. AMO particularly drew attention to [0025] as providing ‘a set of parameters which are said to have been used successfully on a human eye’. It says:
[0025] An example of the results of such a system on an actual human crystalline lens is shown in Fig. 20. A beam of 10 µJ, 1 ps pulses delivered at a pulse repetition rate of 50 kHz from a laser operating at a wavelength of 1045nm was focussed at NA = 0.05 and scanned from the bottom up in a pattern of 4 circles in 8 axial steps. This produced the fragmentation pattern in the ocular lens shown in Fig. 20. Fig. 21 shows in detail the resultant circular incisions, which measured ~10 µm in diameter, and ~100 µm in length.
162. Thus, Figs. 20 & 21 are said to be the results of using a system of the invention, but one using a picosecond laser, on “an actual human crystalline lens” [0024]. Figs. 20 and 21 are very poor quality, and it is difficult to interpret or identify anything other than a series of what would be presumed to be the result of photodisruption bubbles in Fig 20. Even though, in relation to Fig 21, some specific figures are given for the ‘resultant circular incisions’ i.e. that they measured ~10 µm in diameter, and ~100 µm in length, it is impossible to make out what Fig 21 is showing or what the given diameter and length measurements really signify. In any event, [0025] is evidently talking about using a laser to fragment the lens. Although some precision is required to ensure the photodisruption is limited to the lens and no unwanted damage is caused to the capsule, the degree of precision required is less than that required for an AC procedure.
163. Alcon pointed out that neither of AMO’s experts said anything about [0025] in their written evidence. Alcon submitted this was understandable in view of the following points, all of which I accept:
i) [0025] does not say whether the human lens was in vivo or ex vivo. Mr Benjamin’s expectation was the latter. As it turned out, this was not a human lens at all, but a porcine lens, although this would not be apparent to the skilled reader of the Patent(s).
ii) Nothing is said about what imaging was used.
iii) Nothing is said about AC.
iv) There is no suggestion that a reduction in phaco energy was achieved or even tested for, although I suspect the skilled reader would hypothesise that the use of a laser would reduce the phaco energy.
v) There was nothing to establish that the laser and OCT system described would yield any overall benefit to the patient or to the surgeon, although again, I suspect the skilled reader would hypothesise that the system would be of benefit, such that the promises in [0009] would be achieved.
164. Although there is further teaching in the specifications about the imaging system, the passages I have highlighted in [0023]-[0026] plainly indicate that the Patents assume the Skilled Team has the ability, from their CGK, to design and build an imaging system which is able to image the lens capsule and the lens cortex and nucleus in sufficient detail to permit the laser to be focussed as to perform an AC and LF.
165. The patentee gives further details about the relationship between the beam’s properties and the location of plasma formation at [0027]. Alcon submitted this would be CGK and I agree.
166. At [0028], the patentee discloses two alternative methods of applying laser energy in a pattern so as to create a desired cut. [0028] starts by stating in general terms that a three-dimensional application of laser energy can be applied across the capsule along the pattern produced by the laser-induced dielectric breakdown in a number of ways. Sub-paragraph 1) starts by discussing, effectively, producing photodisruption at different depths with a step equal to the axial length of the rupture zone, moving up or down. It goes on to explain the advantages of using a ‘bottom up’ treatment technique, which (a) avoids the laser beam being scattered by bubbles, cracks or tissue fragments prior to reaching the focal point and (b) is said to help protect the tissue underneath the target tissue layer (principally the retina) essentially because the scattering behind the focal point (as it moves upwards) diffuses the energy. Then it suggests there are similar advantages in lens fragmentation by using the ‘bottom up’ approach. Sub-paragraph 2) then discusses four ways of producing axially-elongated rupture zones at fixed points. This discussion may help to explain the dimensions mentioned at the end of [0025]. Since ‘bottom up’ is the additional integer in claim 2 of EP861 and 6 of EP528, I will address this further below.
167. Under the heading ‘Patterns of Scanning’, in [0029] a wide variety of scanning patterns are mentioned. After a reference to the advantages of multifocal focussing and/or patterning systems in lens segmentation, a more general point is made:
‘In addition, these and other 2D and 3D patterns may be used in combination with OCT to obtain additional imaging, anatomical structure or make-up (i.e., tissue density) or other dimensional information about the eye including but not limited to the lens, the cornea, the retina and as well as other portions of the eye.’
168. [0030] returns to consider lens fragmentation. [0031] teaches that complications due to eye movement during surgery can be reduced or eliminated by using very rapid cutting i.e. using a laser repetition rate exceeding 1kHz. I find this was CGK.
169. [0032] has some further general teaching:
‘The techniques described herein may be used to perform new ophthalmic procedures or improve existing procedures, including anterior and posterior capsulotomy, lens fragmentation and softening, dissection of tissue in the posterior pole (floaters, membranes, retina), as well as incisions in other areas of the eye such as, but not limited to, the sclera and iris.’
170. In a passage which I find was also CGK, [0033] states:
Damage to an IOL during posterior capsulotomy can be reduced or minimized by advantageously utilizing a laser pattern initially focused beyond the posterior pole and then gradually moved anteriorly under visual control by the surgeon alone or in combination with imaging data acquired using the techniques described herein.
171. [0034] references the use of an alignment beam (also CGK):
For proper alignment of the treatment beam pattern, an alignment beam and/or pattern can be first projected onto the target tissue with visible light (indicating where the treatment pattern will be projected. This allows the surgeon to adjust the size, location and shape of the treatment pattern. Thereafter, the treatment pattern can be rapidly applied to the target tissue using an automated 3 dimensional pattern generator (in the control electronics 12) by a short pulsed cutting laser having high repetition rate.
172. [0035] and the first part of [0036] are important in terms of the assumptions made by the Patents as to the CGK of control systems:
[0035] In addition, and in particular for capsulotomy and nuclear fragmentation, an automated method employing an imaging modality can be used, such as for example, electro-optical, OCT, acoustic, ultrasound or other measurement, to first ascertain the maximum and minimum depths of cutting as well as the size and optical density of the cataract nucleus. Such techniques allow the surgeon account for individual differences in lens thickness and hardness, and help determine the optimal cutting contours in patients. The system for measuring dimensions of the anterior chamber using OCT along a line, and/or pattern (2D or 3D or others as described herein) can be integrally the same as the scanning system used to control the laser during the procedure. As such, the data including, for example, the upper and lower boundaries of cutting, as well as the size and location of the nucleus, can be loaded into the scanning system to automatically determine the parameters of the cutting (i.e., segmenting or fracturing) pattern. Additionally, automatic measurement (using an optical, electro-optical, acoustic, or OCT device, or some combination of the above) of the absolute and relative positions and/or dimensions of a structure in the eye (e.g. the anterior and posterior lens capsules, intervening nucleus and lens cortex) for precise cutting, segmenting or fracturing only the desired tissues (e.g. lens nucleus, tissue containing cataracts, etc.) while minimizing or avoiding damage to the surrounding tissue can be made for current and/or future surgical procedures. Additionally, the same ultrashort pulsed laser can be used for imaging at a low pulse energy, and then for surgery at a high pulse energy.
[0036] The use of an imaging device to guide the treatment beam may be achieved many ways, such as those mentioned above as well as additional examples explained next (which all function to characterize tissue, and continue processing it until a target is removed)
173. From this point, three particular embodiment systems are described by reference to Figures 11-13. These are a high-level description of various aspects of the system, including its basic architecture in which the imaging device is either an OCT or confocal microscope or where the system uses the same or different lasers for both imaging and treatment. Thus, in [0036] to [0041], three embodiment systems are described by reference to Figs 11, 12 and 13. Fig 11 is a system where the use of a dichroic mirror allows the laser to image and treat. Fig 12 shows an embodiment where the imaging and treatment sources are different. Fig 13 is an embodiment incorporating a confocal microscope. It is only necessary to set out two of these figures and only then to show they show a series of connected boxes:
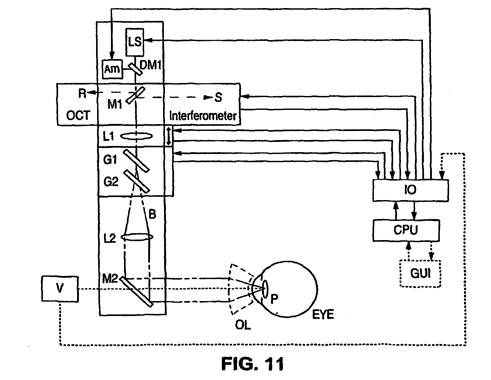
174. In Fig 11, LS is the laser source, AM (or AIM) is an optional aiming beam source, whose outputs are combined using dichroic mirror DM1. The mirror M1 serves to provide both reference input R and sample input S to an OCT interferometer by splitting the light beam B from the laser source. Lens L1 adjusts along the z-axis and when used in conjunction with x and y axis scanning, enables 3-dimensional scanning. XY scanning is achieved using a pair of orthogonal galvanometric mirrors G1 and G2. OL is an optional ophthalmic lens which may also serve to dampen any motion of the eye during treatment. As depicted, it appears to be ‘a conventional eye fixation device’, as mentioned in [0049]. V is optional apparatus for visualizing the target tissue and its output can be displayed on a screen, such as the Graphical User Interface GUI.
175. Towards the end of the description relating to Fig 11, there is this text:
There are many possibilities for the configuration of the OCT interferometer, including time and frequency domain approaches, single and dual beam methods, etc, as described in U.S. Pat. Nos. 5,748,898 ; 5,748,352 ; 5,459,570 ; 6,111,645 ; and 6,053,613 .
176. Since the latest publication of these documents was in August 2000, and because of what I have already found to be CGK as regards OCT, I consider it is safe to assume (and the Patents do so assume) that the ‘single and dual beam methods’ in particular were CGK.
177. By reference to Fig 12, the short passage in [0040] explains the OCT set up when the imaging and treatment light sources are different. The additional components over Fig 11 are: an additional dichroic mirror DM2 which combines the imaging and treatment light; mirror M1 is replaced by beam splitter BS which transmits the treatment wavelength but ‘efficiently separates the light from the imaging source SLD for use in the OCT interferometer’; SLD may be a superluminescent diode, ‘such as the SuperLum SLD-37’. Again, in my view, the Patents assume this form of OCT set up is part of the CGK.
178. Following the description of those figures, there are then short sections on Laser Delivery System, Fixation Considerations, Thermal Considerations and Transverse Focal Volume, concluding with the section entitled Cataract Removal Using a Track and Treat Approach. In these sections, AMO drew attention to the practical information in:
i) The ‘track and treat’ approach in [0042]-[0043], in which an image of the lens is acquired, analysed (automatically or by the surgeon) to produce a cutting pattern, and the cutting pattern is then implemented by the laser and the delivery system. Professor Bouma accepted in cross-examination that this approach was, in effect, image the area you want to treat first and, having imaged it, you then go back and treat the area based on that image, and that was a fairly standard approach to using lasers in a medical context. He mentioned there may be certain instances where you do not need to look in advance, but he accepted the general point.
ii) [0050]-[0052] concerned with assessments of the rise in temperature in the lens material caused by lens fragmentation. Suggestions are made to reduce heating e.g. by cutting the lens into lengths (1x1x4mm) which can still be removed by suction through a needle and which would only result in a temperature increase of 1.04K. In cross-examination, Professor Bouma agreed that this assessment of the temperature rise was GCSE physics.
iii) [0053]-[0054] concerned with avoiding retinal damage via two suggestions: the first being limiting the laser radiant exposure at the RPE (which the skilled reader would understand referred to the Retinal Pigment Epithelium) and the second being reducing the heat exposure during the lens fragmentation. In fact, as was established in the cross-examination of Professor Bouma, the suggestion in [0053] was, in effect, focus the laser where you want to treat and don’t focus it where it might cause collateral damage, ideas that were well within the CGK of the Skilled Team. [0054] refers to a thermal safety limit for near IR-radiation - on the order of 0.6W/cm2. I infer that the Skilled Team would have been aware of this type of figure from work on avoiding phaco burn. Even if that inference is wrong, the Skilled Team would undoubtedly want to ensure no retinal damage, would make rough calculations to estimate the power which would reach the retina and would conduct suitable tests in the wet lab. The rest of [0054] is at GCSE physics level.
179. The control system(s) are mentioned in the Patents at a high level of generality. See the reference to [0035]-[0036] above and the depiction of the controls system by way of example in Figs 11 & 12. Once again, the Patents assume the skilled reader has the ability, using his or her CGK, to design and build these control systems.
180. There are a number of things to note about the disclosure in the Patents:
i) In terms of the practical information provided, the disclosure is of a very wide range of energy levels - from up to 1 µJ to up to 1000 µJ, at pulse durations of 1-3ps and with a repetition rate of between 1kHz and 1MHz, although references to these types of ranges are by no means unusual in patent documents. The specification of course provides specific data to provide a focal spot diameter of 15 µm, and an estimate of the bubble diameter of 48 µm. At best, [0025] provides some dimensions to the ‘resultant circular incisions’, giving a diameter of ~10 µm and length ~100 µm. All of this was established to be CGK or values which the Skilled Team could readily work out using CGK.
ii) The Skilled Team would not rely (or be able to rely) on any of this practical information, unless it coincided with their CGK, without conducting his or her own assessments and/or experiments to confirm the values given in the Patent, not least because of the very poor quality of Figs 20 & 21.
iii) The Skilled Team would be likely to conclude from the disclosure that the patentee had conducted some experiments using a picosecond laser guided by either OCT or ultrasound to generate some cuts in a lens to demonstrate the feasibility of conducting a lens fragmentation procedure. The Skilled Team would note that there is no specific example or indication that an AC procedure had been successfully demonstrated, but, based on the data presented, would accept that such a procedure was plausible.
iv) Much of the detail in [0016] to [0022] was either CGK or, at the very least, the equations and relationships described in those paragraphs were CGK such that the Skilled Team could have worked out the various values presented for themselves and/or verified them by conducting a few basic experiments in the wet lab on pig eyes for example.
v) The “bottom up” approach was the only part of the Patents identified by either of AMO’s experts as being of particular interest or striking. Furthermore, of all the practical information to which AMO drew attention, this remains to be considered. All the rest was established to be CGK, as discussed above.
181. Stepping back from some of the detail, the essential disclosure is of a combination of a sufficiently precise laser used to create incisions in structures of the eye such as the anterior and posterior lens capsule, and in the lens for the purposes of lens fragmentation, the laser being controlled and guided by an imaging system which is able to locate the structures in the eye with sufficient precision. Indeed in [0026], it is suggested that this combination of laser plus imaging system can be used for any ophthalmic procedure which requires incisions to be made in any part of the eye.
182. From what I have reviewed and found above, I now gather together my conclusions as to what the Patents assume as to the CGK of the Skilled Team. The starting point is, of course, that the Patents assume that the Skilled Team have the ability, using their CGK, to put the Patents into effect. At a general level, the Patents assume that the Skilled Team has the CGK and abilities to build or obtain a suitable laser, to create a suitable imaging system and to create a control system by which the eye can be imaged and then the image used to direct the laser pulses to render the desired treatment. In more detail, the Patents clearly envisage the Skilled Team having the following areas of CGK:
i) First, in terms of the characteristics of the laser, the Patents assume the Skilled Team can design and build a sub-picosecond laser system which is capable of delivering pulses which can perform an AC or LF. This is consistent with my finding above that the Skilled Team’s CGK would include femtosecond lasers (as acknowledged in the Agreed CGK set out at paragraph 104 above).
ii) Second, the use of such lasers (plus nanosecond lasers) principally in various ophthalmic surgical applications, including at least PCO (paragraph 107 above), but also the existing methods of treatment.
iii) Third, knowledge of various imaging techniques, including ‘electro-optical, OCT, acoustic, ultrasound’, but it was probable that OCT or confocal microscopy was required if the Skilled Team required a technique sufficient to measure the absolute and relative positions (in a ‘volumetric’ or 3D image - see paragraph 127 above) of various structures in the eye including the anterior and posterior lens capsules, intervening nucleus and lens cortex (see the section on OCT above, and in particular 133 above). Thus, the Patents assume the Skilled Team can design and build an OCT or confocal microscopy system which can image the lens capsule and lens with sufficient precision to enable the laser to be guided to make an AC and to fragment the lens, whether using the same light source for imaging and treatment or separate light sources.
iv) Fourth, knowledge of how to use imaging techniques to ascertain the maximum and minimum depths of cutting as well as the size and optical density of the cataract nucleus (for EP528), to control the chosen measurement and treatment lasers (which may be the same laser operating at different powers) and to automate the operation of the laser during imaging and treatment. Thus, the Patents assume the Skilled Team can design and build a control system which ensures delivery of the laser pulses to suitable focal points so as to perform an AC or LF. Further, that such a control system may be automated and is able to control both a system in which the same light source is used for imaging and treatment or separate light sources.
v) Fifth, how to build test sub-systems and prototype systems embodying suitable laser and imaging apparatus and to conduct tests in a ‘wet lab’.
183. In stating these conclusions, I stress that I am in no way finding that the Patents fail to disclose anything new or inventive. Anticipation is not a ground of invalidity in this case and I have yet to consider the issues of obviousness. At the moment I am simply considering the CGK.
184. In this regard, Alcon’s submission that the disclosure is at a very high level of generality, is essentially correct. In essence, both patents are ‘ideas’ patents. EP861 essentially claims the idea of an OCT (or confocal microscope)/laser system to perform AC and EP528 essentially claims the idea of an OCT (or confocal microscope)/laser system to perform LF.
185. As Prof. Mrochen pointed out in his first report, to implement a system in accordance with the claims, the SE would have to solve numerous technical problems. He said this would have to be done with no assistance from the Patents. I consider his view to be very largely correct. Although the information about the range of pulse energies, focal spot diameters, repetition rates etc place the Skilled Team in the right ballpark, in my view they are either already there or get there in the course of a project. They would already know or could work out these sorts of parameters from their CGK.
186. Whilst Prof. Mrochen’s view was that the notional Skilled Team, with experience in developing ophthalmic surgical systems, could overcome the technical challenges and implement a system in accordance with the Patent claims, the work involved in doing so would not be trivial. AMO’s experts did not suggest that there were any technical challenges that made the Patents non-obvious and, had any such suggestion been made, as Alcon pointed out, the Patents do not solve them.
187. What is not in the Patents also matters. There are no data relating to the safety or efficacy of the claimed system or any specific embodiment (whether in isolation or in comparison to existing techniques) for anterior capsulotomy and/or fragmentation of the lens).
188. The lack of any data is not, in and of itself, an issue. But it applies to one point Mr Benjamin made. He suggested the SO would not contemplate a device in the absence of evidence that it was safe and efficacious. But the Patents do not address such concerns or provide any such evidence. All they do is describe at a high level a system comprising a laser and an imaging device that, it is said, can be used to improve the steps of anterior capsulotomy and phacofragmentation.
189. Claims 1 and 2 of EP861 were said to be independently valid. Claim 1 reads as follows:
|
A |
An ophthalmic surgical system for treating eye tissue by performing an anterior capsulotomy, comprising: |
|
B |
a light source (10, LS) for generating a beam of light (11) comprising a plurality of laser pulses, the beam of light being configured to produce dielectric breakdown at a focal point of the beam of light within the eye tissue; |
|
C |
an imaging device for generating an image of the eye tissue from which a target portion of the eye tissue can be identified, the imaging device being an imaging device selected from a group consisting of an Optical Coherence Tomography (OCT) device and a confocal microscope; |
|
D |
a delivery system (16, L1, G1, G2) for focusing the light beam onto the eye tissue and deflecting the light beam in a pattern, the delivery system including at least one moving optical element for deflecting the light beam in the pattern and for changing the depth of a focal point of the light beam in the eye; and |
|
E |
a controller (12, CPU) operatively coupled to the light source, the imaging device, and the delivery system, and configured to: |
|
E1 |
(a) operate the imaging device to scan the eye tissue so as to generate imaging data for the lens that includes imaging data for an anterior portion of the lens; |
|
E2 |
(b) use the imaging data to determine parameters of a cutting pattern for performing an anterior capsulotomy; and |
|
E3 |
(c) operate the light source and the delivery system to scan the light beam in the cutting pattern, wherein the focal point of the light beam is guided by the controller based on the imaging data so that the laser pulses incise the anterior capsulotomy in the lens capsule, and |
|
|
wherein: |
|
F |
the controller causes the light beam to scan across the eye tissue in the pattern a first time with the focal point at a first depth within the eye tissue and a second time with the focal point at a second depth within the eye tissue different than the first depth. |
190. Despite all the words, the claim is essentially to a system for performing an anterior capsulotomy using OCT or a confocal microscope to image the anterior portion of the lens and to control a pulsed photodisruptive laser which cuts the anterior capsule using photodisruption. This summary may suffice as the inventive concept.
191. AMO provided its version of the inventive concept of claim 1 of EP861 in its Statement of Case on Equivalents, worded as follows (I have slightly modified the numbering):
The inventive concept of claim 1 of EP861 can be summarised as being an ophthalmic surgical system for performing an anterior capsulotomy, comprising
(1) a pulsed laser light source for generating a light beam configured to produce dielectric breakdown within the eye tissue at its focal point,
(2) an OCT or confocal microscopy imaging device for generating an image of the eye tissue,
(3) a delivery system for focussing the light beam onto the eye tissue and deflecting it in a pattern,
each of which is operatively coupled to
(4) controlling means configured
a) to operate the imaging device to scan the eye tissue to generate imaging data for the anterior portion of the lens,
b) to use the imaging data to determine parameters of a cutting pattern for performing an anterior capsulotomy, and
c) to operate the light source and the delivery system to scan the light beam in the cutting pattern with its focal point being guided by the controlling means based on the imaging data to perform the anterior capsulotomy.
192. I have found this useful because it correctly directs attention to the delivery system and the overarching role of the ‘controlling means’, which are necessarily implicit in my formulation.
193. I have also noted that neither my summary nor AMO’s inventive concept make any mention of integer F of claim 1 of EP861. However, Professor Mrochen gave unchallenged evidence that the Skilled Team would be very familiar with the components used to physically control the focal point of the laser. Adjustment of the focal point in the X-Y plane was done much more rapidly by the use of scanners (e.g. galvanometric scanners) than the adjustment of depth of the focal point in the Z axis. For this reason, it was well known by the priority date that in order to minimise the time taken to incise a given 3D cutting pattern using a laser, the most efficient way was to place all X-Y pulses at a given depth Z, before moving to the next depth and repeating all X-Y pulses. In other words, as Professor Mrochen said, this integer does no more than describe the basic and well-known approach as applied to the eye. For this reason, it is not necessary to say anything more about this integer.
194. Claim 2 of EP861 is also said to be independently valid. It limits the system of claim 1 to a bottom up laser cutting system, using these words:
|
|
The system of claim 1, wherein
the controller causes the scanning with the focal point at the first depth to be performed before the scanning with the focal point at the second depth, and wherein the first depth is greater than the second depth. |
195. Claims 1 and 6 of EP528 are said to be independently valid. Claim 1 reads:
|
1 |
An ophthalmic surgical system for creating surgical cuts in an eye having a lens capsule and a lens nucleus within the lens capsule; the system comprising: |
|
2 |
a laser source (10, LS) configured to deliver a laser beam (11) comprising a plurality of laser pulses; |
|
3 |
an optical coherence tomography (OCT) device configured to generate an image of the eye tissue from which the lens capsule and the lens nucleus of the eye tissue can be identified; |
|
4 |
a delivery system for focusing the laser beam (11) onto the eye tissue, the delivery system including one or more movable optical elements, the delivery system operable to focus the laser beam at a focal point within the eye and control the location of the focal point to create cuts within the lens cortex and the lens nucleus; and |
|
5
5A
5B |
a controller (12, CPU) operatively coupled with the optical coherence tomography (OCT) device, the laser source and the delivery system and configured
to determine parameters including upper and lower axial limits of the focal planes for cutting the lens capsule and segmentation of the lens cortex and lens nucleus based on the generated image of the eye tissue and
to control the delivery system to scan the laser beam such that the focal point of the laser beam is scanned in a pattern at multiple depths within the lens cortex and the lens nucleus to segment the lens cortex and the lens nucleus into fragments. |
196. This claim is essentially to a system for lens fragmentation using OCT (or a confocal microscope) to image the lens and to control a pulsed laser which cuts the lens cortex and nucleus into fragments. Again, that summary may suffice as the inventive concept of this claim.
197. AMO’s formulation is worded as follows, which again I have found useful for the same reasons as above:
The inventive concept of claim 1 of EP528 can be summarised as being an ophthalmic surgical instrument, comprising
(1) a pulsed laser light source for delivering a laser beam,
(2) an OCT device for generating an image of the eye tissue from which the lens capsule and lens nucleus can be identified, and
(3) a delivery system which is operable to focus the laser beam and control the location of its focal point to create cuts within the cortex and the nucleus,
each of which is operatively coupled to
(4) controlling means configured
a) to determine parameters including upper and lower axial limits of the focal planes for cutting the capsule and segmenting the lens cortex and nucleus based on the generated image of the eye tissue so that
b) the focal point of the laser beam can be scanned in a pattern at multiple depths within the cortex and nucleus to segment them into fragments.
198. Claim 6 of EP528 is also said to be independently valid. Again, it limits the system of claim 1 to a bottom-up laser cutting system. It reads (with the integer from claim 2 inserted) as follows:
|
|
The system of claim 2 [i.e. The system of claim 1, wherein
the controller is configured to control the delivery system to segment the lens cortex and the lens nucleus into the fragments by scanning the focal point within the lens nucleus in one or more scanning patterns so as to create cuts that separate the fragments]
wherein: |
|
|
scanning the laser beam within the lens nucleus in one or more scanning patterns comprises sequentially applying laser pulses to the same lateral pattern at different depths within the lens nucleus; and |
|
|
the laser pulses are first applied to the same lateral pattern at a maximum depth within the lens nucleus and then applied to sequentially shallower depths within the lens nucleus. |
199. Alcon drew my attention to two general points about these claims. First, whilst EP861 requires a photodisruptive laser and EP528 merely a laser, the claims contain no limitation as to the pulse length. Alcon’s obviousness cases rely on the use of a femtosecond laser, but the claims also cover nanosecond lasers that would produce significant collateral damage in the two applications (AC in particular) and were known to do so in January 2005. Alcon relies on the standard passage from Brugger v Medic-Aid to the effect that a patentee cannot rely on a benefit of his invention that is not achieved across the claim.
200. Second, the apparatus is ‘for’ carrying out the two procedures and the components configured to carry them out. The claims do not require any level of performance. It is on this basis that Alcon submit that if it was obvious to build a device falling within the claim for the purpose of assessing whether the improvements in the three Cs might translate into an overall better outcome for patients, then the claim is obvious. Accordingly, Alcon say that no part of the obviousness analysis requires any assessment of whether there would be any expectation that there would be a benefit over existing techniques. I accept both points and will keep them in mind.
201. Other than those points, no issues of construction were identified.
202. There was a very marked difference between the experts instructed on each side. Alcon called Professor Mrochen to give evidence as to the SE and Associate Professor Lawless to give evidence as to the SO. Here I identify their relevant experience.
203. Professor Mrochen has spent more than 25 years as an engineer, almost all of that time working on engineering and physics-related aspects of ophthalmology. In the course of obtaining his Diploma in Engineering Physics in Germany, he worked at Asclepion-Meditec GmbH in late 1994, a manufacturer of medical lasers which was subsequently acquired by Carl Zeiss in 2002, assisting in developing a control system for the company’s ‘Phacolase MCL-29’, an Er:YAG laser with a handpiece for fragmentation of the lens in cataract surgery. Between 1994 and 1996, he had a role at the University of Jena in Germany concerning optics generally (not involving study of the eye) in which he assisted in building a femtosecond laser used to analyse the characteristics of molecules. Between 1995 and 1999 he studied for a doctorate in theoretical medicine which combined study of laser physics and ophthalmology involving building laser systems for eye surgery including retinal surgery, corneal refractive surgery and cataract surgery (capsulorhexis and lens ablation). His thesis was entitled ‘Erbium: YAG lasers for ophthalmic applications’, such lasers emitting pulses in the nanosecond to microsecond range.
204. Professor Lawless has been a Clinical Associate Professor at Sydney Medical School since 2014. He has more than 35 years of experience as an eye surgeon, specialising in laser vision correction, cataract and lens surgery and corneal transplantation. It is fair to say that Professor Lawless was an early adopter of technology in the ophthalmic field. He has conducted over 30,000 surgical procedures in the following areas: laser corneal refractive procedures (LASIK (performing the second LASIK procedure in Australia in 1995), SMILE and advanced surface laser ablation (ASLA, a modern version of PRK)), manual cataract and lens surgery, laser cataract and lens surgery (also known as femtosecond laser assisted cataract surgery ‘FLACS’) and corneal transplantation. In 1997 he began working for the Vision Eye Institute in Sydney as an ophthalmic surgeon, specialising in cataract and lens surgery, laser eye surgery and corneal transplantation, later being appointed as Medical Director in 2006 until 2016. He has a distinguished record of clinical appointments and leadership roles in prestigious clinical teaching institutions.
205. AMO called Mr Larry Benjamin to give evidence as to the SO and Professor Brett Bouma as to the SE.
206. Mr Benjamin retired relatively recently (December 2019) after a long career as a consultant ophthalmic surgeon at Stoke Mandeville Hospital from 1990, specialising in cataract surgery and diabetic retinopathy but also working in general ophthalmology including corneal transplant, retinal detachment surgeries and squint surgery. Since his retirement he has not undertaken any clinical work but has continued to provide teaching and training on surgical courses at the Royal College of Ophthalmologists and organised various symposia. He had various teaching roles throughout his career, with a focus on ophthalmology, microsurgical skills and complex cataract surgery. He also said he had a great deal of experience with many lasers used in ophthalmology and was involved in running one of the early clinical trials with an excimer laser for photorefractive keratectomy and phototherapeutic keratotomy in the 1990s for a period of five years. He was a medical adviser to Alcon UK between 2000-2012 but only on an ad hoc basis, mainly reviewing clinical advertising or promotional material for compliance with the ABPI’s Code of Conduct. His work did not involve advising on the use of lasers in cataract surgery.
207. Professor Bouma is a Professor of Dermatology and Health Sciences and Technology at Harvard Medical School, also holding faculty academic appointments at MIT and Erasmus Medical Center, Rotterdam and as a Physicist at the Massachusetts General Hospital. His first degree was in physics, with post-graduate work in nuclear physics and a PhD focussed on understanding the interaction of ultrafast lasers with optical materials and plasmas. This was followed by post-doctoral research at MIT in which he continued to work with ultrafast lasers and began to explore their applications in medicine and biology. In 1997 he was offered a faculty position at Harvard. His research lab is in the Wellman Center for Photomedicine at the Massachusetts General Hospital with his focus on the development and clinical application of novel optical technologies for imaging, diagnosis and therapy. Since his time at MIT, he has been deeply involved in the development of OCT, including the first clinical demonstration of OCT in numerous clinical applications and the validation of OCT protocols for the diagnosis of oesophageal cancer and its precursors and the characterisation of coronary artery pathology.
208. To varying degrees, each of the four experts displayed the natural tendency, when pressed in cross-examination, to use their own experience and knowledge as the foundation for what they considered to be the relevant CGK and experience of the SE or SO, as the case may be. I will have to assess the impact of this tendency later and whether each expert managed to adjust to adopt the viewpoint of the ordinary unimaginative person in the art with his or her CGK in mind. AMO submitted that Professors Mrochen and Lawless were far too inventive and knowledgeable, whereas Alcon submitted that Mr Benjamin and Professor Bouma had the wrong SO and SE in mind.
209. The parties agreed that the Skilled Team would be made up of a SO and a SE, and that these two notional persons (the SE might well have been a team of persons) would collaborate in their work. Beyond that, almost everything was in dispute such that when each side referred to the SO or the SE they were effectively talking about notional persons with different experience and knowledge but also, most importantly, with a different level of interaction. This, therefore, is a case where there is considerable interplay between disputes concerning the characteristics of the skilled team and the relevant CGK.
210. In view of the disputes, I start by reminding myself of the summary of the principles concerning the identification of the skilled person or team, as set out by Henry Carr J. in Garmin (Europe) Limited v Koninklijke Philips N.V. [2019] EWHC 107 (Pat) at [85]:
i) A patent specification is addressed to those likely to have a real and practical interest in the subject matter of the invention (which includes making it as well as putting it into practice).
ii) The relevant person or persons must have skill in the art with which the invention described in the patent is concerned. As Aldous LJ stated in Richardson Vicks Inc's Patent [1997] RPC 888 at 895:
"Each case will depend upon the description in the patent, but there is no basis in law or logic for including within the concept of "a person skilled in the art", somebody who is not a person directly involved in producing the product described in the patent or in carrying out the process of production."
iii) The skilled addressee has practical knowledge and experience of the field in which the invention is intended to be applied. He/she (hereafter "he") reads the specification with the common general knowledge of persons skilled in the relevant art, and reads it knowing that its purpose is to disclose and claim an invention.
iv) A patent may be addressed to a team of people with different skills. Each such addressee is unimaginative and has no inventive capacity.
v) Although the skilled person/team is a hypothetical construct, its composition and mind-set is founded in reality. As Jacob LJ said in Schlumberger at [42]:
" ... The combined skills (and mindsets) of real research teams in the art is what matters when one is constructing the notional research team to whom the invention must be obvious if the patent is to be found invalid on this ground."
211. I also take into account the point made by Henry Carr J. in that case at [17]-[18], where he accepted a criticism of the defendant’s expert, that he had selected the wrong team as the skilled addressee because his team did not communicate with each other and that his approach to the prior art was too constrained. The Judge also noted that the approach taken by the expert might have been consistent with the contention that the patent contained an art-changing, Schlumberger-type invention, but that contention had been dropped.
212. Next, I refer to the observations made by Pumfrey J. in Mayne v Debiopharm [2006] EWHC 1123 (Pat) at [3]-[4]:
3. ……Those seeking to enter this field for the first time do not provide what I can call an appropriate template for the skilled addressee, who must represent the attainments of those already in the field in which the invention is made. New entrants to a field may have clearer sight than those already in it, and lack the prejudices properly to be attributable to those with experience. At the same time, a new entrant into the field, albeit a specialist field within his or her general knowledge, will not possess the degree of experience which must also be attributed to the skilled addressee if a proper balance is to be held between the two extremes, of too much stiffness in refusing, and of too much easiness in admitting, any alleged inventive step. It is not sensible not to attribute to the skilled person the common general knowledge of those presently engaged in the manufacture and formulation of platinum-based pharmaceuticals.
4. Mr Waugh QC argues that since the specification enables a wider class of persons - organometallic chemists - to put the invention into effect, then that class of persons is the relevant class. I do not think this follows. After all, obviously the patent is in principle of interest to anybody, whether or not an organometallic chemist, who wishes to enter the field. That fact cannot be relevant to identifying the skilled addressee. It is not legitimate to draw the class of addressee so wide that the specific knowledge and prejudices of those most closely involved in the actual field with which the patent is concerned do not form part of the prejudices and attributes of the skilled person.
213. As Birss J. (as he then was) pointed out in Illumina Cambridge Limited v Latvia MGI Tech SIA [2021] EWHC 57 (Pat) at [63], one of the points being made was that it would be ‘wrong and unfair to the public to define a team so widely that their common general knowledge is so dilute as to make something seem less obvious than it really was.’
214. The importance of identifying whether there were real research teams in the field was emphasised by Kitchin LJ (as he then was) in Medimmune v Novartis [2013] RPC 27 in this passage at [73]-[76]:
73 As the judge explained, in this case there was a dispute as to the identity of the team to whom the patent is addressed. MedImmune contended it is addressed to a team consisting of an immunologist and a molecular biologist, perhaps assisted by a chemist. Novartis argued the patent is addressed to a team of scientists with differing backgrounds in areas such as immunology, in particular antibody structural biology, molecular biology and protein chemistry, but with a common interest in antibody engineering. As the judge identified, the essential difference between the two formulations lies in the degree of specialisation of the team in the field of antibody engineering.
74 The judge preferred Novartis' submission on the basis that the evidence showed that real research teams in the field were teams of the kind contended for by Novartis. He added that, in his view, the specification of the patent is consistent with this characterisation of the skilled team.
75 MedImmune contended that the judge fell into error in so finding because the invention has a broad application and is not confined to antibody engineering. It continued that expertise in immunology and molecular biology is sufficient to implement its teaching.
76 I have no doubt that the judge identified the skilled team correctly. As Jacob L.J. explained in Schlumberger Holdings Ltd v Electromagnetic Geoservices AS [2010] EWCA Civ 819, [2010] RPC 33 at [42], the court will have regard to the reality of the position at the time and the combined skills of real research teams in the art. A little later, at [53], he continued that where the invention involves the use of more than one skill, if it is obvious to a person skilled in the art of any one of those skills, then the invention is obvious. Finally, at [65], he explained that in the case of obviousness in view of the state of the art, a key question is generally "what problem was the patentee trying to solve?" That leads one in turn to consider the art in which the problem in fact lay. It is the notional team in that art which is the relevant team making up the person skilled in the art.
215. Once again, as Birss J. pointed out in Illumina at [68], if it is necessary to address that key question, it is appropriate to rephrase it so its objective nature is clear: ‘what problem does the invention aim to solve?’
216. When I started reading the trial skeletons, it appeared that AMO might be contending that this was a Schlumberger-type case, but the point was not pursued and rightly so. It is therefore not necessary for me to set out the whole of the useful analysis of Birss J. in Illumina at [58]-[71]. In this case I am entirely satisfied that the skilled team to whom the Patents are addressed, and for considering sufficiency, is the same as that for the purposes of considering obviousness. The evidence established that there was an established field, in which real teams operated. I turn to discuss the evidence.
217. Although the entirety of the skilled team is important, it is convenient to start with the characteristics of the SE, the more important member of the team.
218. Professor Bouma’s view of the skilled team was that the Patents are directed to a team consisting of a physicist or engineer with expertise in lasers and imaging (the SE), as well as an ophthalmic surgeon. He was of the view that very few people would have all the skills of the SE, so the SE might well be a team of specialist physicists or engineers who work together to develop laser and imaging systems. He was also clear in his first report that, although the SE would have been aware that lasers and imaging systems were used in medical contexts, including ophthalmology, he or she would not have had a detailed understanding of specific clinical applications of lasers or imaging systems.
219. Professor Mrochen considered that the SE would be a lead product engineer with experience in developing ophthalmic surgical systems. He or she would have, at minimum, a Master’s degree in the physical sciences, in particular physics, optics, electronics and engineering. He or she would have at least 5 to 10 years of industrial experience working in the development of ophthalmic medical technology or perhaps in another medical field involving the use of lasers, alternatively similar experience in an academic research setting. He said the SE would be familiar with the key components and sub-components of ophthalmic laser systems and how they are integrated, including different types of lasers, control elements, delivery systems as well as modalities for the imaging and measurement of ocular structures. The SE would also have an understanding of the anatomy of the eye, of laser-tissue interactions and a general appreciation of common ophthalmic disorders and surgical techniques used to treat them.
220. Professor Mrochen also considered that the field of ophthalmic technology was an international one, with much sharing of information at key international conferences in the industry. He identified a number of key players in what he called the ophthalmic laser space at the Priority Date including some 11 named companies, (including both AMO and Alcon), some of which were acquired by AMO and Alcon after the Priority Date. There were both large ophthalmic technology companies (like AMO, Alcon and Carl Zeiss Meditec) and a number of smaller companies seeking to develop and commercialise ophthalmic technologies or devices. He also identified a number of key universities and research centres operating in the ophthalmic technology space at the Priority Date, including 5 in Germany, 1 in Austria, 2 in the US (including MIT) and 1 in Switzerland. He also named some 16 key researchers in the field, the publications of which he said would be followed with interest by the SE, and whose names appeared on textbooks and papers.
221. In terms of the SE, although AMO criticised Professor Mrochen’s evidence because they contended he was too inventive and too knowledgeable (points I address below), his evidence relating to those operating in the field was not challenged and I found it entirely convincing. I find there were real life teams operating in this field at and before the Priority Date.
222. Furthermore, in my view Professor Mrochen was better qualified by far than Professor Bouma to give evidence about the attributes and knowledge of the SE in this case. In his first report, although Professor Bouma included a substantial section setting out topics he considered to form part of the CGK, this material was almost entirely theoretical, albeit relevant. He did not identify any sources of CGK, other than the general experience of his notional SE - an undergraduate degree in physics, applied physics or electrical engineering and at least some postgraduate training in laser or optical engineering with expertise in optics, laser engineering, signal processing, image processing and computer coding of control algorithms. In line with his experience with OCT, he was able to give details as to what OCT systems were available and when in the lead up to the Priority Date, but there was no equivalent practical information from the engineering side of the ophthalmic technology field. As Professor Mrochen pointed out in his second report, it was not clear whether Professor Bouma’s SE had any practical, industry experience in the development of medical lasers, active medical devices or ophthalmic medical technology. That was a restrained observation, because it became clear that Professor Bouma was working on the basis that his SE required no such practical experience. His SE was able to develop and build a femtosecond laser for use in an ophthalmic application from scratch, along with its imaging system, either OCT or confocal. I found this approach entirely unrealistic. It was, however, consistent with his (and AMO’s) approach to CGK - that there were no written sources of CGK information.
223. When Professor Bouma was questioned about whether something was or was not CGK, it became clear to me that (matters relating to OCT apart) he was not able to answer based on any experience in the field of the development of ophthalmic surgical systems, but he gave his answer based on an assessment of whether he thought it should or should not be CGK, that assessment being very largely based on what he had learned during his involvement in this case. In short, Professor Bouma was unable to provide me with any reliable evidence on the CGK (again, OCT apart).
224. There was a second major problem with Professor Bouma’s evidence. It was apparent from Professor Bouma’s written evidence that he took a restricted view of the characteristics of the Skilled Team, and the SE in particular. During his cross-examination, it quickly became apparent that Professor Bouma had misunderstood the characteristics and abilities of the Skilled Team or Person. The extent of his misunderstanding emerged in cross-examination. He was asked to consider the skilled team working to design, develop and make ophthalmic surgical devices, with the Skilled Team reading Mühlhoff together. It was suggested to him that the Team would be interested in looking for new clinical applications for the equipment taught in Mühlhoff. In that context, in a striking answer, he made it clear he viewed the role of the SE as having ‘a practical interest in the topical matter of in this case the specification. So their job is to put into practice that invention, to build that instrument to make it work.’ (my emphasis). By contrast he said ‘I think it is the job of a professor to innovate and to find new opportunities and to invent’. Slightly later, in the context of the SE reading the reference in [0015] of Mühlhoff to other applications, it was suggested to him that the SE would ask the SO about incisions in the lens. Again, his answer was revealing:
10 A. Not in my experience. The way that the skilled engineer works
11 is the skilled engineer is busy applying the subject matter of
12 the invention to build an apparatus. They are not innovators.
13 They are not going out and, you know, trying to find new
14 inventions. They are building devices. I distinguish that
15 really profoundly from the role of an academic, the role of an
16 innovat[or], the role of an entrepreneur. It is a very different
17 responsibility.’
225. From those answers, I gained the clear impression that Professor Bouma approached the question of obviousness on the basis that the SE would not do anything new because his job was to implement a specification presented to him and build the device described in it. Similarly, Professor Bouma seemed to me to equate doing anything other than implementing a specification as invention.
226. Mr Benjamin took the view that the SO would be a consultant ophthalmologist with a significant portion of their practice dedicated to cataract surgery. He set out a conventional route to such a position, via various stages of training, specifying that by the time of achieving consultancy, the candidate would have performed a minimum of 350 cataract procedures. Later in his CGK section, Mr Benjamin gave an account of when various procedures were developed and available, including RK (developed in the early 70s but surpassed by the Priority Date by the newer operations), PRK (early 80s), LASIK (first performed 1990), LASEK (first performed 1999) and femto-LASIK (in which a femto-second laser was used to cut the corneal flap prior to the use of the excimer laser to ablate the cornea in LASIK). Mr Benjamin was doubtful that the average UK ophthalmologist would have been aware of femto-LASIK at the Priority Date although he accepted it was possible that those with a speciality in refractive surgery might have been aware of the early cases. He explained this was partly due to the fact that refractive surgery was only available privately in the UK and not generally on the NHS. It was not entirely clear whether Mr Benjamin’s SO would have been merely aware of these developments or would have had practical experience with the equipment in question. It was also not clear whether Mr Benjamin’s SO had prior experience in developing a new ophthalmic surgical system with a SE. I strongly suspect he or she did not.
227. Professor Lawless agreed that the SO would be a surgeon with experience in cataract surgery, albeit that would not be his or her sole focus. He explained that most ophthalmologists practice as ‘generalists’ and see patients with a variety of different conditions. He considered the SO would also have experience in the use of lasers in ophthalmology, with a basic understanding of laser physics. He would have used a variety of lasers in clinical practice. He also made two particular points. First, that this field was global in outlook, and gave several examples to demonstrate the sharing of knowledge, information and experience across a global community of ophthalmologists at meetings, via publications in the scientific and medical literature and via personal communications between fellow ophthalmologists. Second, as to the degree of interaction between the SO and the SE. Having participated himself in the development and implementation of new medical devices for ophthalmic surgery, he had relevant experience of working with engineers and developers.
228. In view of the parties’ different positions on the characteristics of the SO, I asked Professor Lawless about the adoption of technology by ophthalmologists. His answer was it was reasonably accepted that about 10% were early adopters, about 10% were laggards and around 80% are in the middle and fairly consistent, such that once the early adopters have sorted out new technology, they take up new technologies fairly quickly.
229. Professor Lawless had previously accepted he was an early adopter, as he clearly was, an attitude consistent with his actual involvement in development projects. Mr Benjamin was not an early adopter and I think it would be fair to characterise him as in the middle group i.e. a potential user of new technology but only after it had been become established via the early adopters. Indeed, from listening to Mr Benjamin giving his evidence, I gained the distinct impression that he viewed the SO as largely a user of equipment as opposed to someone actively involved in developing it. His SO would give advice to the SE when asked for it, but I got the impression his SO would have that somewhat detached role.
230. In my view, the SO in the team would be drawn from the pool of early adopters but would also have had experience of developing and implementing new medical devices for ophthalmic surgery. He or she would also have had the experience of lasers which Professor Lawless described. Those characteristics would, in my view, be required for the SO to play his or her role in implementing either of the Patents.
231. My conclusion in this regard is supported by the evidence from Professor Mrochen as to the real-world teams working in this area, as summarised above.
232. Although I acknowledge Mr Benjamin did have some experience with lasers in ophthalmic applications, his experience was somewhat dated by the priority date because he was not actively involved in developing ophthalmic surgical systems (as opposed to using commercialised devices). In general, I am inclined to place more reliance on the evidence from Professors Mrochen and Lawless.
Interaction between the SO and the SE
233. One of the curiosities in this case was that, despite the agreement that the SO and SE would collaborate, on Alcon’s side their two experts were kept firmly separate. This emerged in the course of cross-examination on particular passages in the expert reports which were either identical or very nearly so. Although each expert was given a final or near final draft of the other’s report to read, they were not allowed to communicate at all. The result was that any ‘communication’ between the two experts took place via what the solicitors chose to tell them. This had the further consequence that certain important passages in the respective reports were identified in cross-examination as being identical. Thus some of the critical words with which each expert gave his ultimate conclusions on obviousness were effectively the same. I have no doubt that each expert firmly believed what was set out in his report. Thus, I conclude that the identity in the language used was the result of the solicitors summarising discussions using the same words.
234. When solicitors are endeavouring to develop expert evidence in accordance with the Medimmune guidance, it is understandable that they seek to exert tight control over the process. However, that control ought not, in my view, to be allowed to interfere with the development of a necessary part of the expert evidence. Real life teams in this field, when developing systems of this nature, would have been engaged in a potentially lengthy and complex project which would have proceeded through a number of stages, including: initial concepts and outline design and (if the concept and design were considered to be worth taking forward) development of prototype sub-systems (e.g. laser system, control, measurement/imaging) and testing, more detailed system design, development and testing, assembly and testing of overall system. The level of collaboration would vary considerably though the stages but I have no doubt that the collaboration would be intense when initial concepts and outline design were under consideration. In view of the obviousness issues in the particular circumstances of this case, it is that stage which is critical.
235. Accordingly, the fact that Professor Mrochen had to develop his views without the benefit of face-to-face discussion with Professor Lawless (and vice-versa) interfered with the presentation of the expert evidence in this case. I will have to assess the impact of this but, from my viewpoint, I think the primary effect was to create difficulties for each of them in cross-examination.
236. So far as the position on AMO’s side is concerned, it is necessary to distinguish between issues of disclosure as opposed to issues of obviousness.
237. On issues of disclosure, there does appear to have been a high degree of coordination between Professor Bouma and Mr Benjamin. If they had considered disclosure from their individual viewpoints of SE and SO respectively, I doubt that they would have managed to arrive at the same points. None of this really matters, because I have reached clear views on the disclosures of Freedman and Mühlhoff respectively and I happen to have concluded in each case that both Professor Bouma and Mr Benjamin failed to treat each document fairly.
238. However, when it comes to considering issues of obviousness, the position is different. When I re-read the particular paragraphs in the experts’ reports of Professor Bouma and Mr Benjamin where each of them addressed the issues of obviousness, it was clear to me that each of them had considered the issues purely from the viewpoint of their SE and SO respectively.
239. So far as Professor Bouma is concerned, this point emerges very clearly from two (very similar) passages in his first report, first when considering Freedman and second, Mühlhoff:
‘The Skilled Engineer would not have any knowledge of the treatment of cataracts and so would not have the idea to modify Freedman to perform treatment of the lens, nor would the Skilled Engineer regard it as within their competence to make any decisions about whether to consider modifying the device of Freedman to treat eye tissue other than the cornea. I understand that Mr Benjamin will be considering, in his report, this question from the perspective of an ophthalmic surgeon.’
‘… - the Skilled Engineer would not have any knowledge of the treatment of cataracts, nor would the Skilled Engineer consider it within their competence to make any decisions about modifying Mühlhoff to perform any other procedure. Again, I understand that Mr Benjamin will be considering, in his report, this question from the perspective of an ophthalmic surgeon.’
240. There is nothing in Professor Bouma’s second report to indicate he changed this approach.
241. When one turns to Mr Benjamin’s reports, it is clear that Mr Benjamin does indeed consider these issues from the perspective of an ophthalmic surgeon. In fact, it is clear from his reports that Mr Benjamin addresses all issues of whether a particular step was obvious solely from the perspective of his SO.
242. The effect of this evidence is clear: on AMO’s side of the case, the SE and SO did not interact at all. This conclusion is a further reason why the evidence from Mr Benjamin and Professor Bouma on obviousness is expressed on an incorrect basis.
243. From my viewpoint, it appeared that each side’s position on the relevant characteristics of the Skilled Team largely reflected the experience of their experts. The most substantial issue was concerned with whether the SO and SE would have practical experience of developing surgical systems, in particular those employing lasers in ophthalmic surgical applications. As the trial progressed, it became ever clearer to me that AMO’s experts approached this case on the basis that the SO and SE did not require any such prior practical experience. As I have indicated, Mr Benjamin saw his SO as essentially a user of ophthalmic equipment and Professor Bouma had no experience in this field. In that sense, they were coming to this field as newcomers. Furthermore, although lip-service was paid in AMO’s evidence and submissions to the notion that the SO and SE would interact, as I have already said, I was able to detect almost no trace of interaction in the reasoning presented by Mr Benjamin or Professor Bouma. At times on a particular topic, one did defer to the other, but that is not what I consider to be interaction.
244. The approach taken by Professor Bouma and Mr Benjamin - essentially that the SO and SE were newcomers to the field - infected the whole of AMO’s case, including the approach taken in cross-examination of Alcon’s experts. This skewed the evidence in this case to an extent which is illustrated by the fact that Alcon saw the need to proffer alternative submissions in closing which I have found to be unnecessary.
245. Despite everything I have said above, I am satisfied that, from the expert evidence as a whole, the Court has been sufficiently educated as to the knowledge and characteristics of the Skilled Team.
246. As I indicated, the Technical Background section above was very largely based on the Statement of Agreed CGK which I received after the trial. However, I found the Statement of Agreed CGK rather dry and theoretical, lacking real indications of the sort of practical knowledge which real-life people in this art would have possessed. The few additions I did make in the Technical Background section concerned that type of practical knowledge.
247. By the time of Closing Submissions, there remained very considerable dispute over the CGK, and in a very real sense, the disputes over CGK lie at the heart of this case. Very considerable proportions of the closing submissions were dedicated to a detailed debate on CGK. After the trial the parties agreed a list of CGK issues which remained in dispute. Some of them overlap or interact and they vary in their specificity. As a result, I have found it necessary to address nine topics below which I introduce briefly here:
i) Sources of CGK.
ii) The nature of this field.
iii) Whether there was a perceived need to improve the two parts of cataract surgery in issue here namely, anterior capsulotomy and phacoemulsification, plus the more general perception of whether ‘automation’ would improve accuracy, precision and reproducibility of treatment.
iv) Refractive surgery and femto-LASIK.
v) The use of lasers in ophthalmology, specifically: where the development of lasers suitable for use in ophthalmic surgical procedures had got to by the priority date. This included the use of lasers in refractive and other ophthalmic procedures. One particular issue which arose in this general area was whether previously unsuccessful attempts to use lasers in ophthalmic surgical applications could be CGK. The argument here was how could failed attempts be characterised as ‘a good basis for further action’.
vi) Turnkey femtosecond lasers.
vii) OCT and its use in ophthalmic applications and specifically what was CGK as to how accurately OCT or another imaging technique could image the components of an eye.
viii) The SE’s CGK of OCT.
ix) Control of lasers in ophthalmic surgical systems.
248. A striking feature of this case is the fact that AMO’s experts identified virtually no sources of CGK. In his first report, Mr Benjamin referred to one or two papers on specific points plus 2 timelines which I believe were supplied to him by AMO’s solicitors. As far as I could see, Professor Bouma identified no sources of CGK in his first report.
249. In his second report, Mr Benjamin responded to a number of Professor Mrochen’s suggestions (which were, of course, as to CGK of the SE) from the perspective of his SO. The only common ground was as to the Dodick use of a Nd:YAG laser as an alternative to phacoemulsification and the Wavelight Er:YAG laser to break up the lens nucleus. In his second report, there was some rather grudging evidence from Professor Bouma that (i) the SE in industry would read Laser Focus World but he cast doubt on whether the SE would read the specialist engineering and physics-related journals identified by Professor Mrochen, and he rejected the notion that the SE would read any of the specialist ophthalmic journals identified by Professor Mrochen; (ii) the SE might attend some of the Conference on Lasers and Electro-Optics (‘CLEO’) and conferences held by the OSA and by SPIE, primarily because those conferences were accompanied by trade fairs at which manufacturers would exhibit optical components, laser systems, diagnostic equipment, control systems etc.
250. Professor Bouma indicated he was familiar with just some of the names identified by Professor Mrochen as being key researchers and groups in the field, and rejected the idea that the SE would follow all publications from particular individuals. He said it was more realistic to say that the SE would be aware of the headline results of certain individuals: Professor Bouma gave Dr James Fujimoto as an example and his paper in Science which described the first results in OCT. This was a landmark paper in 1991, but was in no way representative of CGK in January 2005.
251. This summary explains the nature of most of the issues on CGK. Although Mr Benjamin, Professor Bouma and AMO participated in agreeing the Technical Primer and the Statement of Agreed CGK, they volunteered almost no sources of CGK. As I said, there was some grudging acceptance of a limited number of Professor Mrochen’s identified sources. In submissions AMO challenged the remaining sources of CGK which Professor Mrochen had identified, saying that Alcon simply had not proved any of the information was CGK. In this regard, I have well in mind that Mr Benjamin’s experience was not representative of the SO, and Professor Bouma, despite his expertise in OCT, was not in the relevant field and similarly was unable to assist on the CGK of the SE. Of course, had AMO called expert witnesses who were more in touch with the experiences of the SO and SE, I strongly suspect that AMO would have found it much more difficult to dispute CGK to the extent that they did. As a major company in the field, I am sure that AMO would have been able to locate and instruct experts who were more in tune with real-life teams at around the Priority Date than Professor Bouma in particular.
252. Before addressing these disputes, it is necessary to set out the applicable principles. Naturally, each side referred to the oft-cited passage of Arnold J. (as he then was) in KCI v Smith & Nephew [2010] EWHC 1487 at [104]-[112] (as approved by the Court of Appeal [2010] EWCA Civ 1260 at [6]), itself often summarised (as it was by AMO in this case) as ‘To be CGK, information must be generally known to the bulk of those in the art, and generally accepted as a good basis for further action.’ This summary focusses on ‘positive’ CGK which is often the exclusive focus in many patent cases.
253. However, there are cases where, for want of better expressions, what I might call ‘intermediate’ and ‘negative’ aspects of CGK are relevant.
254. The prime example of ‘intermediate’ CGK is Merck v Ono [2015] EWHC 2973 (Pat), where Birss J. (as he then was) was faced with an issue as to whether contradictory reports relating to the nature of a particular pathway in immunotherapy could be CGK. Having referred to KCI, in [23] he pointed out that the phrase ‘generally regarded as a good basis for further action’ derives from the Court of Appeal in General Tire v Firestone [1972] RPC 457 and was preferred by the Court to Luxmoore J’s ‘accepted without question’. He continued at [24]:
‘I do not believe the court in General Tire was seeking to address factual circumstances like those said to arise in this case. In principle the common general knowledge of a skilled person must be capable of including contradictory ideas on a topic, always assuming that information reaches the standard for common general knowledge. The existence of a defined area of doubt and uncertainty does not mean that, in principle, such knowledge is not part of the common general knowledge. An example, referred to by Ono, was in the judgment of Floyd J in Regeneron v Genentech [2012] EWHC 657 (Pat) e.g. at paragraph 67 and the conclusion at paragraph 88 (upheld by the Court of Appeal at [2013] EWCA Civ 93, paragraph 22). Merck submitted the evidence in Regeneron was much stronger than the evidence in this case. The submission about evidence does not alter the point of principle.’
255. For ‘negative’ CGK I have in mind the archetypal ‘mindset’ case - Dyson v Hoover [2001] EWCA Civ 1440. In that case the first instance judge (Mr R.M. Fysh QC as he then was) described the industry as ‘bag-ridden’, a phrase expressly approved by Sedley LJ. Aldous LJ said the Judge was entitled to make the findings in this paragraph and, to my mind, thereby approved it:
"156. … Common general knowledge has both positive and negative aspects. I have so far considered under this topic, as is customary, only positive aspects of the knowledge with which the skilled addressee is to be imbued. In my view in certain cases (and I believe this to be one of them), negative aspects of knowledge must in approximation to reality, play their part. At the priority date of the Patent, I believe that such was the 'mindset' within the vacuum cleaner industry, no notional, right-thinking addressee would ever have considered the viability of purifying dirt-laden air from a vacuum cleaning operation, other than by means of using a bag or bag and final filter. For present purposes, the addressee is nonetheless deemed to have been presented with (in effect) three items of prior art wherein it is proposed to clean dirt-laden air by means not of bags but by cyclonic action alone. He is also assumed to take some interest in them however inimical the proposals may be to his likely way of thinking at the time. In terms of its impact on the issue of obviousness, I believe that this negative thinking which as Mr Kitchin suggested amounted to prejudice, would at least have caused the addressee to regard modification to any of these prior art proposals with considerable reserve if not overt scepticism. This likelihood must, I consider, be given due weight. In my view of the matter, I cannot think that any of the cited prior art would ex facie be likely to have lead the addressee at the relevant date with any enthusiasm to effect the often substantial changes which would bring these proposals within a claim of the Patent: see para 153. My view in this regard is bolstered (but not precipitated) by Mr Dyson’s evidence of what actually happened when he tried to interest the industry in Dyson I."
256. Like Birss J., I consider the previous general formulations (KCI and General Tire) do not address the precise factual circumstances which arise in this case. Whilst I entirely accept the KCI paragraphs, some of the issues which emerged in this case demonstrate it is not a complete statement of the law.
257. Since AMO contended that Professor Mrochen in particular had strayed far beyond what was CGK, I also reminded myself of a key passage in the judgment of Pumfrey J. in Horne Engineering v Reliance [2000] FSR 90 at [13]-[14]:
13. ….it is important to bear in mind the warning of Aldous LJ. in Beloit Technologies Inc. v. Valmet Paper Machinery Co. Ltd [1997] RPC 489 at 494, he said this:
It has never been easy to differentiate between common general knowledge and that which is known by some. It has become particularly difficult with the modern ability to circulate and retrieve information. Employees of some companies, with the use of libraries and patent departments, will become aware of information soon after it is published in a whole variety of documents; whereas others, without such advantages, may never do so until that information is accepted generally and put into practice. The notional skilled addressee is the ordinary man who may not have the advantages that some employees of large companies may have. The information in a patent specification is addressed to such a man and must contain sufficient details for him to understand and to apply the invention. It will only lack an inventive step if it is obvious to such a man.
It follows that evidence that a fact is known or event well-known to a witness does not establish that that fact forms part of the common general knowledge. Neither does it follow that it will form part of the common general knowledge if it is recorded in a document.
14. Aldous L.J. said that in order to establish whether something is common general knowledge, the first and most important step is to look at the sources from which the skilled addressee could acquire his information." I would add that although it has to be remembered that a specification may fail to provide sufficient details for the addressee to understand and apply the invention, and so be insufficient and invalid, it is often possible to deduce the attributes which the skilled man must possess from the assumptions which the specification clearly makes about his abilities.’
258. In terms of sources of CGK, AMO also drew attention to the further reminder in the judgment of Meade J. in Merck, Sharp & Dohme v Wyeth [2020] EWHC 2636 at [85]-[86] that not all textbooks and not all scientific articles, let alone all their contents, can be taken to be CGK without proof as to their reach, impact and acceptance.
259. Likewise, the previous general formulations do not address the precise factual circumstances which arise in this case, and specifically, whether previous attempts to employ lasers in ophthalmic surgery and which did not gain acceptance could be CGK. For the purposes of analysis, I will assume this type of attempt can be characterised as a failure, even though in practice, the position is somewhat more complicated.
260. In his first report, Professor Mrochen described this field as a small one in terms of the personalities involved who were working either in industry or in academia, were known to each other, would regularly attend the same annual conferences and would read the same types of industry publications. He said the main sources of CGK for the SE at the priority date were commercial products, academic journals and industry publications, reference texts and industry or academic conferences. He nominated a wide range of journals including Ophthalmology, the Journal of Refractive Surgery, the Journal of Cataract & Refractive Surgery and Investigative Ophthalmology & Visual Science and Optical Engineering, the Journal of Biomedical Optics and the Journal of Medical Imaging.
261. In terms of textbooks, he identified Steinert (Cataract Surgery: Techniques, Complications, Management. 2nd Edition, 2004) as a source from which the SE would have been aware of developments, and he exhibited Chapter 51 by Jack Dodick and Julia Katz entitled ‘Lasers in Cataract Surgery’ (‘Dodick’ – see further below). In his more general discussion, he noted that reference texts tended to be a few years behind the curve in terms of reflecting developments in the field, given the fast-moving nature of the field.
262. No doubt because it was apparent from the first expert reports from AMO that CGK was going to be in dispute, Professor Mrochen exhibited extracts from three further textbooks to his second report. These were:
i) A chapter entitled ‘Ultrafast Lasers in Ophthalmology’ by RM Kurtz and MA Sarayba in Ultrafast lasers - techniques and applications (Marcel Dekker, Inc., 2003) (‘Kurtz’). The preface states ‘Ultrafast Lasers is intended for researchers, engineers and graduate students who are interested in a review of ultrafast optics technology. … This book addresses the reader who is interested in a summary of the unique capabilities of ultrafast lasers.’
ii) A chapter entitled ‘Ophthalmic Applications’ by H Lubatschowski and A Heisterkamp in Femtosecond Technology for Technical and Medical Applications (Springer, 2004) (‘Lubatschowski’). The book is part of the Springer series ‘Topics in Applied Physics’, a series ‘addressed to all scientists at universities and in industry who wish to obtain an overview and to keep abreast of advances in applied physics. The series also provides easy but comprehensive access to the fields for newcomers starting research.’
iii) In Chapter 4 ‘Medical Applications of Lasers’, section 4.1 entitled ‘Lasers in Ophthalmology’ by MH Niemz in Laser Tissue Interaction: Fundamentals and Applications (2nd Edition, Springer 2002). (‘Niemz’). In his preface to the first edition (1996), the author wrote ‘Due to the rapidly increasing number of medical laser applications, it is almost impossible to present a complete survey of all publications. Thus, this book will mainly serve as a starting guide for the newcomer and as a quick reference guide for the insider. For discussion of the newest techniques and results, the reader should consult the latest issues of scientific journals rather than a textbook. Regular coverage is provided by the journals Lasers in Surgery and Medicine, Lasers in Medical Science, Biomedical Optics, and the SPIE Proceedings on Biomedical Optics. Apart from these related articles frequently appear in special issues of other journals e.g. Applied Physics B and the IEEE Journal of Quantum Electronics as well.’ In the preface to the second edition the author indicated he had taken new developments into account. In particular he said the contents of chapter 4 - the chapter on applications - strongly depends on the current state of the art.
263. Mr Benjamin did not accept that Steinert was CGK, on the basis that it was not a routine text used in the UK. Two chapters from Steinert are referred to (and incorporated) in the Background section of the Patents - Chapter 15: Principles of Nuclear PhacoEmulsification, and Chapter 44 which appears to relate the relatively primitive technique requiring a high degree of manual dexterity on the part of the ophthalmic surgeon performing PCO using a Nd:YAG laser with a series of high energy pulses in the range of 1 to 10 mJ ‘manually marked out on the posterior lens capsule’ giving an opening with a coarse nature.
264. AMO accused Professor Mrochen of doing a literature search to put himself in the shoes of the skilled person and to find and establish CGK. AMO also complained of the textbooks referred to and exhibited by Professor Mrochen in his second report, submitting they had been put there by the Professor as a ‘reservoir’ of knowledge, into which he could reach when pressed in cross-examination. More generally, AMO submitted that Professor Mrochen had not properly understood the concept of CGK.
265. Professor Mrochen was subjected to a robust and searching cross-examination. I gained the impression that he was genuinely taken aback at being challenged on some rather basic matters of practical knowledge which he regarded as CGK. As a result he became somewhat defensive in his answers. I consider it was a natural reaction for him to refer to the textbooks which he had exhibited in order to support his view that something was CGK. I do not think he can be criticised for that. As I have indicated, his views were far more closely aligned to the extensive CGK which the Skilled Team required to operate in this field.
266. It is true that Professor Mrochen referred to having conducted a literature search, but he said he did this in order to put himself back into the position which existed at the Priority Date. This is a perfectly legitimate approach, provided that the results of that literature search are not assumed to be CGK without further consideration.
267. AMO levelled less severe criticisms against Professor Lawless’ evidence, but they included criticism as to the level of knowledge of the IntraLase machine.
268. AMO criticised the way in which Alcon put various allegedly CGK documents to Mr Benjamin and Professor Bouma in cross-examination. Generally, the criticism was that Alcon had not established the document or content was CGK and did not do so by the way they were put in cross-examination.
269. In terms of sources of CGK, I broadly accept Professor Mrochen’s evidence, but only up to a point. In so finding, I accept one of AMO’s criticisms that Professor Mrochen had difficulty at times in distinguishing between what was known and what was CGK. It would be an invidious task to make findings on every point in dispute, but the extent of my acceptance of each side’s points will appear from the following.
270. So far as textbooks are concerned, I find that the Steinert chapter represented the level of CGK in this field in the UK, even though the book itself was not in routine use in the UK. I find that the Kurtz, Lubatschowski and Niemz extracts were also properly representative of CGK in the UK by the Priority Date, based, in each case, largely on the content of each extract, but also on the intended readership, into which the Skilled Team fell very squarely. Although AMO made strenuous submissions to the effect that Alcon had wholly failed to establish these extracts were CGK, I do not understand how a Skilled Team could operate in this field without the content of those extracts forming part of their CGK, in particular because those extracts provide much practical information which is almost completely absent from the Statement of Agreed CGK or confirm it, to the extent it was included.
271. I also find that the SE in particular would have ensured s/he kept up to date with developments by reviewing at least some of the journals cited by Professor Mrochen. His list was more focussed on ophthalmology than those listed by Niemz in his preface, but that is because Niemz was attempting to cover all medical applications of lasers. Niemz’s general point remains a good one: in a fast-moving field, a textbook is out of date as soon as published, so it is necessary to review the latest papers to keep abreast of the latest developments. I am satisfied this was a field in which the Skilled Team would do just that.
272. In view of the extent of the CGK which was agreed and the necessarily wide scope of it, AMO’s stance in challenging these textbooks as representative of the CGK was entirely unrealistic. These were just the sort of textbooks which the SE would have on his or her bookshelf at work.
273. I will address the status of any individual papers further below. Professor Mrochen may not have always understood or had in mind the somewhat subtle distinction between (a) a paper itself being CGK and (b) the main point or content of a paper representing CGK. Often he was being challenged as to the former when in practice he was really saying the latter. In my view, what he was trying to convey was an impression of the considerable amount of practical knowledge and experience which the SE had to have had in order to work in this field. The Agreed CGK is all very well, but it really represents the theoretical basis for the work of the Skilled Team and omits a vast amount of practical experience which the Skilled Team would have had.
274. Although this was only addressed indirectly, I consider it assists to have in mind the nature of the field in which the real-life teams were working around the priority date. This was very much a research and development field. Once a product had been developed, the manufacture was relatively straightforward but there was evidence that a project to develop a new ophthalmological laser surgical system for clinical use would take a number of years of effort - perhaps as much as 5 to 7 years, starting from scratch and including obtaining regulatory approval.
275. This is reflected in some of the content of the textbooks I have discussed above.
276. As I understand matters, the Dodick Photolysis system was first demonstrated in 1991, yet in Steinert, published in 2004, it was relevant for the creators of that system to write extensively about their system, as well as the Phacolase MCL-29. Both products are discussed with reference to a whole range of research papers.
277. It is apparent that the discussion in Kurtz is concerned with applications for femtosecond lasers which are ‘already in clinical use and/or commercial development’ and each is discussed with reference to a significant number of research papers. Niemz discusses both established procedures and those still being researched, both by reference to research papers dating back several years, often to the 1980’s or 1990’s. Similarly, the discussion in Lubatschowski.
278. These textbook extracts demonstrate that the Skilled Team would be left years behind the art if they waited for commercial devices to appear, let alone become accepted by ophthalmologists generally. In order to keep abreast of developments to enable them to function in this art, the Skilled Team had to be aware of the matters discussed in these textbooks and, I find, would also have been aware of the significant research papers published in this field, but not all published papers. The significant research papers can be identified by the regularity with which they are cited in these textbooks and/or by reference to the research groups in question. To the extent that it matters, I identify these in relation to specific topics below.
279. Manual cataract surgery comprised four steps (i) initial incision, (ii) anterior capsulotomy, (iii) lens fragmentation and removal and (iv) IOL insertion. Of those, (ii) and (iii) were regarded as being the most difficult steps. Mr Benjamin considered that consultant ophthalmologists ought to be able to achieve all the steps relatively straightforwardly, but he acknowledged that in his book he had said that some consultants still consider the capsulorhexis to be the most challenging part. It is clear that it takes years of training and experience (both in the wet lab and on real patients) to reach consultant level - the evidence was that a minimum of 350 procedures is required and this is often exceeded in practice.
280. It is also clear that a significant proportion of cataract surgeries were conducted by junior doctors at the priority date. A 2004 paper by Muhtaseb in the British Journal of Ophthalmology reported that of a 1000-patient sample, around 2/3 had been operated on by junior doctors and 1/3 by consultants, with a complication rate of 2.8% across the whole sample. Mr Benjamin referred to another study which suggested only 1/3 of patients were operated on by junior doctors. The precise proportion does not matter because it is clear that an individual patient might well not be operated on by a consultant, and even consultants experienced problems.
281. Turning to the AC procedure itself, CCC was the standard procedure at the priority date. A good AC was one that was circular, centrally located and the correct size (the three C’s). Whether these three requirements were met depended on the skill of the surgeon and the anatomy of the patient, because some patients had features making it more difficult or even impossible to achieve a good capsulorhexis. Following cross-examination, it was agreed that all three of these requirements played a role in a stable IOL placement and reducing the risk of PCO. Correct placement of the IOL reduced the incidence of PCO as the capsular bag would wrap around the IOL - the ‘cling wrap’ effect. Furthermore, a good AC was necessary to benefit fully from more sophisticated IOLs, since, for example, multifocal lenses were more sensitive to issues caused by decentration and tilt.
282. I find that Chapter 7 of Mr Benjamin’s 2007 book represents a good indication of the position as at the priority date of the CCC technique. As Mr Brian Little (the author of that particular chapter) put it:
‘Probably the most important 60 seconds of any phaco operation is the time spent in creating a central and circular rhexis of the correct size. It sets the stage for the rest of the operation.’
283. More than half of the chapter is devoted to discussing capsule problems and complications. Professor Lawless cited a complication rate of around 2% for experienced surgeons and 5% for trainees, relying on the Muhtaseb paper. Mr Benjamin said those rates were too high, but he relied on the somewhat lower complication rate of Dr Robert Osher from the US, who was well-known and accepted to be a good surgeon. As Mr Benjamin accepted, even a complication rate of 1% represented a large number of individuals, whether in the UK or worldwide.
284. At the priority date, I find that CCC was a critical step in cataract surgery and the evidence established that a tear could lead to a cascading set of serious consequences, including the following:
i) If the tear extended to the posterior capsule, causing vitreous loss, that could result in severe permanent visual loss, prolonged visual recovery and the need for subsequent surgeries.
ii) Even where an anterior tear did not extend to the posterior capsule, it could still have a serious impact on the ability to fit an IOL properly, causing errors in accuracy and issues of vision quality.
iii) It was inevitable that anterior tears would happen from time to time. When answering a question about obviousness over Freedman (a topic I address later), Professor Lawless said this:
24 A. No, I do not agree. I think that that ophthalmologist back in
25 2005, the centre of his surgical life was cataracts. If he
2 was doing 10 cataracts a week, which would be pretty typical,
3 he would be getting a problem every five weeks, a problem of
4 capsular rupture that would seriously impact the patient and
5 him or her. That is a problem. That is why surgeons were
6 always trying to make things better, and that would be front
7 and centre of that doctor's mind. It is just, I think,
8 reasonable to think, "Well, here is an image-guided laser.
9 This is great. Let us try this, and obviously it is going to
10 be a Femto; we will do it inside the eye. Let us at least
11 attempt to go down this path with an engineer". To me it is
12 self-evident, knowing what is in the mind of a regular
13 ophthalmologist who does a lot of cataracts, what he would be
14 thinking in 2005.
285. In his Chapter 7, Mr Little explained the potential seriousness of capsular tears:
“There is one of these complications above all others that warrants more detailed discussion because of its particular importance, and that complication is a radial tear-out (Fig. 7.5)…We can describe it as a radial extension of the capsulorhexis tear. This gives an acronym (RECT) that phonetically describes its potential effect (i.e. wrecked) on the surgical outcome”
286. In his written evidence, Mr Benjamin indicated that the SO would not see any need to improve on CCC. However, in cross-examination, his views moved to being much more aligned with those of Professor Lawless. I accept that the SO might have had a concern about a new technique deskilling trainees but I find that the SO knew that the CCC technique was not perfect and s/he would have been interested in a technique that had the potential to improve the accuracy of the AC, reduce the risk of tear-outs and would also have been interested in a technique that might make things easier for trainee surgeons, provided it was an addition rather than a replacement for the CCC technique. So, in summary, whilst the motivation to find a better AC technique was not overwhelming, the SO would nonetheless have been interested in any technique that promised to improve accuracy and reduce the risk of tear-outs.
287. In addition, the discussion in evidence about complication rates very much related to the situation in first-world economies like the UK, the US and Australia. However, I consider the Skilled Team operating in the UK might well have in mind developing apparatus that could be used in less developed countries, where I infer there was a or a perception of greater unmet demand for cataract surgery.
288. In terms of the lens fragmentation step, Professor Lawless described it as a fiddly procedure. The introduction of phacoemulsification had enabled small incisional extracapsular surgery, but it came with significant risks of phaco burn, tissue damage caused by acoustic shock or by surgical manipulation of the phaco probe. By the priority date, numerous techniques were in play to attempt to reduce the risks of phacoemulsification, including fragmenting the lens using a scalpel or the phaco probe itself before the application of ultrasonic energy (e.g. ‘phaco chop’ and ‘divide and conquer’).
289. Again, Mr Benjamin’s written evidence was that the existing procedure was safe, effective and repeatable ‘in the hands of a trained practitioner’. Professor Lawless’ view was that it remained a difficult step in cataract surgery and one that ophthalmologists were actively trying to improve. By way of support for his view, Professor Lawless referred to the program for the ASCRS/ASOA Symposium on Cataract, IOL and Refractive Surgery held in May 2004. He was challenged on this in cross-examination:
21 Q. We have not seen anyone expressing the view in any of these
22 papers in the case that there was a need to find an
23 alternative technique?
24 A. Well, the AquaLase is an alternative technique, it is cited
25 twice here in just one page. That is an attempt to find an
2 alternative technique to phaco. It did not play out in a way
3 that was successful over a few years, but they were trying.
4 They were trying because people wanted to make it better.
5 That is why they were sitting through meeting after meeting
6 with these -- this emphasis on cataract surgery and trying to
7 make it better.
290. Furthermore, as Alcon submitted, if there was no desire to improve on phacoemulsification, why was it being discussed at this symposium at all.
291. Mr Benjamin sought to downplay the risk of phaco burn but he conceded there was a risk of posterior capsule rupture caused by manipulation of the phaco probe within the capsular bag. I find that phaco burn remained a concern at the priority date. Whilst for the experienced surgeon, phacoemulsification was relatively straightforward, Mr Benjamin agreed the procedure was not perfect, so there was room for improvement. Even in 2007, it is clear from Mr Benjamin’s book that ophthalmologists embarking on their training were still being warned about phaco burn and ‘what not to do’, and confirms it remained a matter of concern. Steinert referred to the risk of phaco burn and identified a number of devices which were intended to supplement or replace conventional phacoemulsification devices, including the Dodick and Asclepion-Meditec laser devices, of which the SO would have been aware.
292. The Dodick photolysis system comprised a Nd:YAG nanosecond laser fired at a titanium plate to create shockwaves which ruptured the lens material. The Asclepion-Meditec device was an Er:YAG photoablating laser directed to the lens by an optical probe. It was common ground that both were slow and incapable of breaking down the lens nucleus sufficiently, so the surgeon would have to revert to traditional phacoemulsification in any event.
293. Again, in summary, I find the SO at the Priority Date would have been interested in a new lens fragmentation technique that avoided the risks of phaco burn (in particular by reducing the phaco energy) and of posterior capsular rupture. The point I made in paragraph 287 above applies equally here.
294. The refractive surgery techniques of RK, PRK, LASIK and LASEK were all CGK of the SO. In particular, LASIK was part of the SO’s CGK by the Priority Date. It was one of the laser-based procedures that had replaced RK and was therefore an example of a laser technique that was more reliable and safer than the former manual technique. The issue was whether femto-LASIK, in which a femtosecond laser was used in place of a mechanical microkeratome to create the corneal flap, was also CGK of the Skilled Team.
295. Mr Benjamin’s view was that since the benefits of femto-LASIK were still being investigated in 2006, the technique could not have been CGK in January 2005. However, I am satisfied that his view was based on a wrong appreciation of the SO and what qualified as CGK. Furthermore, the weight of the evidence was to the contrary:
i) Femto-LASIK machines had been approved both in the US and in Europe and were commercially available. They were programmed and able to perform LASIK flap creation, corneal tunnels and cutting of the host tissue in corneal transplants. Professor Lawless took delivery of an IntraLase machine in October 2004.
ii) IntraLase, the company which developed femto-LASIK, had a high market profile by the Priority Date, as evidenced by some market scope reports from OMP.
iii) There were multiple papers discussing femto-LASIK published in ophthalmic journals, including papers by Nordan (2003), Ratkay-Traub (2003) (which Professor Lawless described as ‘key’), plus Kezirian (2004) and Binder (2004). I find the SE would have read both Nordan and Ratkay-Traub.
iv) Femto-LASIK was being discussed widely at ophthalmological conferences both in the US and Europe and was referred to in a 2003 textbook Custom LASIK Surgical Techniques and Complications, where Chapter 24 LASIK flaps with the femtosecond laser was written by Ratkay-Traub, Kurtz, Juhasz and Nordan, some well-known names in the field.
v) Professor Lawless referred to it as a ‘hot topic’ at the time. The IntraLase machine was being exhibited and demonstrated at conferences. Alcon even managed to unearth a Daily Mail article from September 2004 reporting on ‘scalpel-free surgery’ being used by an NHS surgeon in East Grinstead.
296. In cross-examination of Professor Lawless, AMO made a sustained attempt to establish that femto-LASIK was not CGK. Various suggestions were made: that femto-LASIK was not a commercial success by the priority date - but that misses the point; that commercial sales were limited to the US - but the OMP documents disprove that; that most ophthalmic surgeons would not have had practical experience with the IntraLase device by the priority date - which was true, but again misses the point that femto-LASIK was a ‘hot topic’ and the details of how it worked were pretty simple. As Professor Lawless said ‘You cut a flap. You have been doing that since the 1990s with a mechanical device, and then you replaced it with a laser. There was not a lot to know.’
297. AMO suggested that the papers I listed above were tentative in their conclusions or had flaws in their methodology, but I accept the general tone of Professor Lawless’ evidence that the message was that femto-LASIK was a good technology that reduced the complication rate observed with mechanical microkeratome flap creation. For example, the Nordan 2003 paper showed significant benefits for flap predictability and preservation of epithelial integrity, as Mr Benjamin agreed.
298. Overall, I was entirely satisfied that femto-LASIK formed part of the CGK of the SO. I also find that femto-LASIK was part of the CGK of the SE, to the extent that it matters. There were multiple references to femto-LASIK in the textbooks exhibited by Professor Mrochen including in Kurtz, Lubatschowski and Niemz (Indeed, Niemz includes a striking high magnification photograph of a femto-LASIK treatment). When some of these were put to Professor Bouma, all he could say was that this was outside his direct experience.
299. Alcon submitted the significance of femto-LASIK was as follows:
i) First, that it was an example of an ophthalmic surgical procedure in which a laser capable of photodisruption was in use before the priority date.
ii) Second, it was an example of a femtosecond laser used as a replacement for a surgical knife to increase the precision, accuracy and reproducibility of a procedure.
iii) Third, it was evidence of a femtosecond laser instrument having been developed even where the existing procedure (using a mechanical microkeratome to cut the flap) was considered generally acceptable.
300. Furthermore, in the Ratkay-Traub 2003 paper, it was suggested that the femtosecond laser could be put to good use for other ophthalmological applications, including cataract surgery. In the final part of the discussion section, the authors said this:
Femtosecond lasers may also have significant potential for improving corneal transplantation surgery (anterior, or posterior lamellar and full-thickness transplantation), as well as surgical manipulation of other ocular tissues, such as the sclera (glaucoma surgery) and the lens (cataract surgery or presbyopia correction). Continuous improvements in ultra-fast laser technology and the increasing demands from ophthalmologists to improve available surgical techniques suggest that the femtosecond laser in refractive surgery will evoke further investigation.
301. A similar point was made at the end of the Kurtz chapter in Ultrafast Lasers. Having discussed the basics of laser-tissue interaction, the chapter discusses femtosecond laser surgical applications in the cornea. It concludes with a short section on ‘Other ophthalmic applications’ which starts ‘Other obvious targets include the rest of the transparent ocular tissues (lens, capsule and vitreous) as well as surgical procedures in translucent tissues such as the sclera. …’ and in the Conclusions ‘The minimally invasive, high-precision characteristics of femtosecond laser technology make it highly promising for various ophthalmic surgical procedures. A number of initial applications in the cornea are already in clinical use and/or commercial development.’
302. Of course, I remind myself that not every statement in an individual paper or textbook chapter is CGK, even if the main topic - femto-LASIK - is CGK. However, I consider that the type of statement that I have just quoted were properly representative of the view of the Skilled Team as regards the potential of femtosecond lasers. In other words, there was a ‘buzz’ in the art about femtosecond lasers. More generally, I find that the Skilled Team well appreciated that the femtosecond laser was a tool which enabled the making of very precise incisions inside the eye, without an incision from outside the eye.
303. As Alcon submitted, there was considerable common ground between the experts as to the use of lasers in ophthalmology (the issue of femto-LASIK apart, which I have just resolved). The following uses were CGK:
i) The use of a Nd:YAG laser for PCO. This was a nanosecond laser, controlled through a slit lamp. Professor Lawless’ evidence was that this laser was good, cheap and effective and ophthalmologists had them in their offices. Professor Mrochen said this revolutionised the treatment of PCO and was a true milestone in laser medicine. He also characterised it as still one of the most performed ophthalmologic procedures using a laser. He agreed that as at 2005 it was the only success story in the history of attempts to use lasers to carry out procedures on the lens.
ii) The use of a Nd:YAG laser in the Dodick Photolysis system for lens fragmentation in cataract surgery.
iii) The use of a photoablative Er:YAG laser (the Asclepion-Meditec Phacolase 29) for lens fragmentation in cataract surgery.
iv) The use of photoablative excimer lasers for corneal surgery in PRK, LASEK and LASIK.
v) The use of Nd:YAG lasers for glaucoma treatment and retinal surgery.
All the Nd:YAG lasers identified above were photodisruptive.
304. The big issue was whether some of the historical attempts to use lasers in cataract surgery were (i.e. had remained) CGK at the Priority Date, in particular for AC and lens fragmentation or lens softening.
305. Dr Jack Dodick and Dr Julia Katz wrote Chapter 51 of Steinert (2nd Edition, 2004) entitled ‘Lasers in Cataract Surgery’ in which they described their Dodick Photolysis system, the Phacolase system and made some predictions for the future. Their chapter starts with a historical review of the attempts to use lasers in cataract surgery, including the attempts in the 1980’s to use Nd:YAG lasers for AC and, in the late 1980’s, for softening the lens prior to phacoemulsification. They comment that due to various complications (including converting one stage surgery into two stages), neither procedure gained widespread acceptance. It is apparent that this Chapter was not a full survey of all uses of lasers in cataract surgery. Their primary focus was plainly on phacoemulsification or, more generally, lens removal.
306. AMO accepted that the use of excimer lasers and Nd:YAG for PCO were CGK. Those apart, AMO submitted that the CGK was limited to the existence of the Dodick system and the Phacolase, how they operated in general terms, that they were slow and unpopular and that there was nothing in that CGK to encourage the use of lasers in cataract surgery.
307. I find the historical attempts at a general level were part of the CGK, partly because they are referred to in Steinert, Kurtz and Lubatschowski, and partly because if they were not CGK, then both the Skilled Team (and real-life teams) would be condemned to repeat, from time to time, the mistakes of the past e.g. attempting to use a nanosecond laser for AC. Niemz (2002) does not explicitly discuss the historical attempts but does suggest picosecond pulses are advantageous for fragmentation of the lens because of the lower threshold energy required for optical breakdown compared with nanosecond lasers. In addition to the reasons set out in the textbooks, the Skilled Team either knew or would be able to find out, as part of their CGK, why these historical attempts failed: for both AC and LF, albeit in different ways, it was because nanosecond lasers were too powerful and the risk of collateral damage was too high. To my mind, that raised the question as to why such lasers proved successful for PCO. Although this question was not addressed directly in evidence, it appears that procedure could cope with the power of the Nd:YAG nanosecond laser pulses with no real occurrence of collateral damage (provided the pulses were not fired directly at the IOL), possibly because it is not just the posterior capsule that has to be cut, but also the additional scattering membrane that is the cause of the problem. Also, the retina is relatively distant. PCO requires much less precision than an AC. Niemz describes the procedure as one where the surgeon places several line cuts, whereupon the posterior membrane ‘opens like a zipper’.
308. In any event, in order to operate in this field, I find that the Skilled Team (and the SE in particular) would need to have a detailed understanding of the ranges of operating conditions of nanosecond through to femtosecond lasers in ophthalmic applications at a level which is summarised in these tables from Kurtz and Lubatschowski respectively. These provide more detail than in the Agreed CGK:
309. It is relevant to note, as is pointed out in Kurtz, that between nanosecond and femtosecond lasers, the pulse duration is decreased by six orders of magnitude, and Lubatschowski spells out the range in pulse energy between ns and fs lasers.
310. Furthermore, I find that the Skilled Team would have practical experience of applying laser pulses into ophthalmic tissue (human, bovine or porcine) to make incisions. Part of the reason for this is because of the types of optically transmissible material in the eye, in which the effects of lasers are different to other tissue in the body.
311. I find it was also CGK as to why, for example, attempts at AC using nanosecond and picosecond lasers did not prove successful. It was because the laser pulses were too powerful and caused collateral damage, also giving rise to the complications noted by Dodick, a rise in intraocular pressure and inflammation, as well as others - the edges produced by nanosecond pulses were too rough. This is a piece of ‘negative’ CGK but with a positive component, because it was part and parcel of a long-running general desire to find applications in ophthalmic procedures where lasers might prove successful. This long-running desire stemmed from the ability (demonstrated, for example by Nd:YAG PCO) for lasers to make incisions in the eye without any other intervention. However, the failed attempts to use nanosecond lasers for various applications meant that those in the art were waiting for the further development of lasers which effected photodisruption using less energy. By the priority date, the Skilled Team knew that femtosecond lasers were available and had established themselves for femto-LASIK.
312. This piece of ‘negative’ CGK stemmed from one or more of the papers by Puliafito and Steinert (1984), Vogel (1994), Aron-Rosa (1984) and Chambless (1985). These papers were frequently referred to in the textbooks and the Skilled Team would have looked at these papers if they wanted to find out more information beyond the summaries in the textbooks. In this regard, I agree (again up to a point) with Professor Mrochen that the Skilled Engineer would have kept an eye on papers being published by some of the well-known groups in the field, again in order to keep abreast of developments. These groups included Puliafito and Steinert, Vogel, and Lubatschowski.
313. Having said all that, I must also take account of the fact that Professor Mrochen exaggerated the extent of use of picosecond and femtosecond lasers. In his first report, when addressing obviousness over Mühlhoff and Freedman, he relied on this summary of the CGK position:
‘In particular, as I described in paragraphs 107 to 114, the use of ultrashort pulse lasers (picosecond and femtosecond lasers) to cut lens capsule and tissue inside the lens would have been known to the Skilled Engineer.’
314. However, his paragraphs 107-114 certainly did not support such uses of femtosecond lasers. For uses of picosecond lasers to fragment or soften the lens, Professor Mrochen relied on essentially experimental work (e.g. by Puliafito and Steinert, Vogel and others) but his point is also supported by the reference in Niemz to picosecond pulses being advantageous for fragmentation of the lens and specific mention of a picosecond Nd:YLF used for fragmentation. In terms of attempts to use picosecond lasers to cut the lens capsule, he did not cite anything in this section and in fact I have found that the earlier experimental attempts (e.g. Vogel 1994) established that picosecond lasers had not proved successful or worth taking forward for AC.
315. To the extent that I am wrong as regards the content of the specific papers I have mentioned above being CGK, I also find that, when embarking on any project in this field, the Skilled Team would undertake a literature search for research previously directed at the application in question. Such a search would have identified the papers I have mentioned, at the very least.
316. Due to AMO’s very determined resistance on matters relating to the CGK, having made these findings I again reviewed the guidance I have set out above in order to check I had not strayed beyond what was properly CGK. However, as I have indicated above, I do not understand how a Skilled Team could operate in this field without the level of knowledge I have indicated above. The fact that AMO drew its battle line far from where my findings have ended up is simply a consequence of their case being detached from the real-world position.
317. To summarise, I find that the Skilled Team would know, as part of their CGK, that low picosecond but more so, femtosecond lasers were well worth looking at for making incisions inside the eye. Fragmentation of the lens was a less demanding application in which picosecond lasers had been shown to work in experimental work. However, AC was a more demanding application in which picosecond lasers were still too powerful. The SE would know (as part of his CGK) that femtosecond lasers were likely to prove capable of use for making incisions inside the eye.
318. There are three final and more general points on the use of lasers in ophthalmology. One is concerned with the mechanisms of action. AMO drew a sharp distinction between those lasers which produced an ablative effect, which they said was confined to a surface treatment, and those which effected photodisruption. Any blurring of this distinction was treated by AMO as heresy and AMO levelled significant criticism at Professor Mrochen for suggesting in his cross-examination that an ablating laser could include a laser operating to remove tissue from below a surface. I find this criticism was misplaced. Professor Mrochen had mentioned in his first report studies exploring the use of excimer lasers to ablate the lens whilst keeping the capsule intact. In addition, when he was challenged in cross-examination he pointed out the passage in Niemz that discusses intrastromal ablation. Furthermore, although I was not supplied with Chapter 3 of Niemz, I note from the Table of Contents that it covers a variety of interaction mechanisms which are not limited simply to photoablation and photodisruption. I am not at all sure this matters, but I find that the SE would have been aware of other mechanisms of action of lasers in tissue. In my view, AMO’s case to the contrary merely emphasised the lack of involvement of Professor Bouma in this field. Whether all the research which Professor Mrochen referred to in his evidence was CGK is a separate point, which I have dealt with (to the extent necessary) above.
319. The second point is illustrated by the PhacoLase. At some date (and it does not matter when it was) the development of the PhacoLase was technically obvious, yet it did not prove to be a commercial success because the improvement it offered over the ophthalmologist’s existing ultrasound machine for phacoemulsification was not sufficient to displace that machine, bearing in mind the additional cost of the PhacoLase. The point is that, in this particular field, a machine or system might well not be developed because of commercial concerns or not prove successful, even though the development of that system was technically obvious.
320. The third point concerns the sizes of the photodisruption bubble created by various pulsed lasers. These are indicated in the tables I have reproduced above from Kurtz and Lubatschowski. The Skilled Team would know that the gas in these bubbles takes time to be absorbed by the surrounding tissue, and it can be minutes depending on the size of the bubble. Kurtz draws a distinction between the use of nanosecond lasers and femtosecond lasers, but makes a particular point about cutting direction in this passage, which I find to represent CGK for the SE/Skilled Team:
‘Owing to their large collateral tissue effects, nanosecond ophthalmic photodisruptors have mainly been used to create explosive tears in surgical targets far from delicate structures. The best example of such an application is posterior capsulotomy, performed to disrupt the opacity that develops in the optical path behind the plastic intraocular lens, after cataract surgery (Steinert and Puliafito, 1985). In contrast the localised effects of femtosecond disruption described in the previous section permit its use as a highly precise cutting tool. To be used in this manner, essentially as a remote-controlled scalpel, individual laser pulses must be placed contiguously creating a postage stamp effect that results in incisional planes within the tissue. These planes can be placed in any or any orientation to create horizontal vertical or oblique incisions (Fig 1).
Tissue targets that are transparent to the laser wavelength allow optical breakdown to occur at any depth or location without affecting tissue outside the photodisruption zone. For targets in the eye, this generally restricts laser wavelengths of the visible and near infrared. The only limitation to creating arbitrary incision planes is that they must be written from the deepest portion of the tissue to the shallowest coma because static gas bubbles that persist in tissue shadow the laser if the focus is moved to a plane below previously produced bubbles. Using a femtosecond laser with high pulse repetition rates (in the kilohertz range) and a computer-controlled scanning optical delivery system, localised micro photodisruptions can be placed in a contiguous fashion to produce incisions of any shape to produce high precision tissue separations. Complex shapes can also be created by intersecting these resection planes.’
321. I base that finding on the experience which the Skilled Team would have in testing various pulsed lasers on ophthalmic tissue to create incisions. In my view they would have experienced the problem of gas bubbles shadowing the laser. AMO’s strong resistance on this point was essentially based on the SE coming to the field as a newcomer without practical experience.
322. This particular issue was an attempt by AMO to create a foundation for the question ‘If it was obvious, why was it not done before?’ This attempt failed.
323. AMO put to Professor Mrochen two femtosecond laser systems which they suggested had been commercially available from the early 1990s and were ‘turnkey’ i.e. suitable for clinical application. These were the ‘Mira’ and the ‘Tsunami’. Neither was ‘turnkey’ or suitable for use in the ophthalmology clinic at the priority date. The ‘Mira’ had a lengthy start-up routine which included verification of the power output using a suitable power meter and an oscilloscope. A version of the Tsunami was described as ‘turnkey’ by the manufacturer, but it was not launched until 2009.
324. As appears from the CGK section above, it was common ground that OCT was part of the Skilled Team’s CGK by the Priority Date. It was a known imaging technique and commercial OCT devices were in use in clinical practice for particular applications. Those used in the clinic for cataract surgery in 2005 were relatively basic, essentially allowing measurement of the distances between cornea, lens and retina but the SO would have known of more sophisticated OCT devices that were being used to produce detailed images of the posterior segment of the eye for the purposes of diagnosing and treating glaucoma and macular disease.
325. The dispute between the parties was whether or not the SO would have known that OCT was suitable for imaging the lens, and in particular whether OCT had the necessary resolution to do so. Alcon contended this dispute was irrelevant for the following reasons:
i) First, the relevant CGK is that of the Skilled Team, not just that of the SO. Alcon contend that the SE would have known that OCT was capable of imaging the lens with axial resolution of just a few microns - I consider this in the next topic.
ii) Second, Alcon pointed out that both pieces of prior art disclose the use of OCT to image the anterior structure of the eye. This is something of an exaggeration which I will assess in the context of each piece of prior art.
iii) Third, Alcon submit that if, as was put to Professor Lawless several times in cross-examination, the CGK was that OCT was incapable of imaging the lens with appropriate resolution, then the Patents would be insufficient. Alcon point out that the Patents simply assume that OCT can image with the necessary resolution. At best, the Patents assert that ‘It is believed…’ in essence that OCT is capable. No data is presented to prove the validity of this belief.
iv) The Patents assume that the Skilled Team have the necessary degree of skill to make an OCT device with appropriate resolution to image the lens capsule and the lens so that a laser can be directed to make appropriate incisions in both and the Skilled Team therefore has the same degree of skill in the context of the validity attacks.
326. I agree that this dispute is not relevant to the issue of what was CGK and I will proceed on the basis of the third and fourth points in particular.
327. However, AMO had criticisms of the reasoning of both Professor Lawless and Mrochen on this OCT issue, which I must discuss because they form part of AMO’s wider criticism that the approach of both experts was tainted by hindsight.
328. In his first report, Professor Lawless relied on knowledge of “the successful use of OCT to take high quality images and measurements across the whole eye (including the anterior segment)” and awareness of “the ability of OCT to yield accurate, high resolution images of the anterior segment of the eye, and in particular the lens’. These points were set out in his CGK section and repeated in support of his reasons on obviousness.
329. In his CGK section, Professor Lawless relied on an image from a Carl Zeiss Visante machine (reproduced from a 2010 paper), but in cross-examination he accepted that the Visante machine was not launched until after the priority date (around October 2005) and also Zeiss’ claim that it was ‘the first [OCT machine] to provide clear, highly detailed, in-depth images of the anterior chamber’. AMO submitted that even in the Visante image the position of the anterior capsule was not shown, but I disagree - it can be seen. Professor Lawless maintained however that ‘there was a sense that it was capable of giving them those images. It was just a matter of time..’ It is right to record that Professor Lawless did refer to other technologies as well, including the Pentacam device and the SL-OCT device launched by Heidelberg Engineering in 2003. He included two Scheimpflug images from a Pentacam device showing the lens and a nuclear cataract, but he said the original Pentacam device launched in 1999 was not useful for anterior segment or lens assessment. Although Heidelberg Engineering was a recognised company in the field, the information about the capabilities of the SL-OCT device was almost non-existent. In essence, I agree with AMO’s submission that the material provided by Professor Lawless did not support his proposition.
330. This is the more relevant knowledge because the SE would have had greater and more detailed knowledge of the capabilities of OCT than the SO, and knowledge going beyond commercially available machines.
331. I have summarised the Agreed CGK in relation to OCT above, but some additional points emerged from the cross-examination of Professor Bouma.
i) First, Fourier-domain OCT had been demonstrated to be better than time-domain OCT in 2003, and allowed a significant increase in scanning speed.
ii) From 2003 onwards, Fourier-domain OCT devices were subject to a continual process of development and speed improvement.
iii) Although the first Fourier-domain OCT devices were not on the market until after the priority date, the SE was able to make and implement a Fourier-domain OCT device at the priority date with axial resolution in the single-digit micron range.
iv) OCT devices had been used from early on to try to image the anterior segment of the eye, as evidenced by the Izatt 1994 paper. This was a seminal paper which I find was CGK for the SE. It contains some striking images of the anterior segment of both human and bovine eyes, produced using OCT. The date of the Izatt paper is an example of a general trend in this field: there can be as much as a decade (or more) between the first research article and the emergence of commercial devices utilizing the identified principle.
v) OCT devices were in use for imaging the back of the eye (indeed OCT devices were originally developed for retinal imaging).
332. Furthermore, the point made in sub-paragraph 325.iv) above applies here. The SE would know or expect that OCT or confocal microscopy had those imaging capabilities.
333. However, I return to the point made in paragraph 327 above. In his first report, Professor Mrochen cross-referred to the relevant section of Professor Lawless’ first report (which I have discussed above) but added a few additional observations from the perspective of the SE. In relation to OCT, his main additional points were as follows:
‘OCT: In the years leading up to the Priority Date, and since the launch of the first commercial OCT systems (for imaging of the retina) in the 1990s, OCT technology had improved markedly, enabling higher resolution imaging and more precise and accurate measurements of the relative positions of structures in the eye. A range of different OCT-based imaging and measurement systems were launched in quick succession in the late 1990s and early 2000s from Zeiss and others, including the first OCT systems designed for biometry and imaging of the whole eye and anterior segment (as opposed to focusing on the retina). At the Priority Date, OCT would have been regarded as a highly promising imaging technique that now offered appreciably better axial resolution, precision and accuracy than competing technologies around that time, and that was continuing to improve.’
334. The first sentence was correct. The second sentence emulated what Professor Lawless had said and suffered from the same flaws. Not unnaturally, Counsel for AMO cross-examined Professor Lawless on this aspect and not Professor Mrochen. This approach however did not deal with or challenge Professor Mrochen’s third sentence. What Professor Mrochen was there saying was in effect that the SE would think that OCT could be used to image the lens capsule and lens with sufficient precision (even if a commercial device was not yet available).
335. In my judgment, this was a justifiable statement based on (a) what was shown in the 1994 Izatt paper and (b) the very significant developments in OCT since then, even if a commercial device which used OCT to image the anterior segment (including the lens capsule and lens) was not on the market by the priority date. In view of the long time lag between proof of concept and the launch of a commercial device in this field, this conclusion is also supported by the launch of the Zeiss Visante machine in October 2005. In other words, the SE would have expressed no surprise at all if told at the Priority Date that a commercial device capable of imaging the anterior segment, including the lens capsule and lens was to be launched in a few months time. Its capability would have been what they expected to be able to achieve at and before the Priority Date.
336. Although this was not identified by the parties as being a CGK point in dispute, it is necessary to discuss this topic briefly. When preparing this judgment I was struck by the absence of evidence as to what was CGK on how laser ophthalmological surgical devices were controlled, and in particular what techniques the Skilled Team had for ensuring that when the laser pulses were first fired at eye tissue they were fired in the right place. From the totality of the evidence, I have gleaned the following.
337. First, it was common practice to fixate the eye either using an applanation lens or below a suction ring with a contact glass plate on its top (as illustrated in Figure 5 of Lubatschowski). This provided a fixed point of reference for the focal plane of the laser, so control of laser procedures involving incisions in the cornea (e.g. for RK, PRK, LASEK, LASIK and femto-LASIK), was relatively straightforward.
338. For PCO, Niemz explained:
‘Usually, a helium-neon laser is used as an aiming beam. The surgeon first focusses this laser on the posterior capsule and then adds the cutting Nd;YAG laser beam as shown in Fig 4.6 by pressing a footpedal. Typically pulse durations of 30ns, pulse energies of up to 5mJ and focus diameters of 50-100 µm are used. With these laser parameters, local power densities exceeding 1010 W/cm2 are achieved, leading to the phenomenon of optical breakdown as described in Sect. 3.4. After having placed several line cuts, the posterior membrane opens like a zipper as illustrated in Fig. 4.7. The whole procedure can be controlled through a slit lamp. The surgeon’s eye is protected by a specially coated beamsplitter.’
339. The use of a slit lamp and a HeNe aiming beam were also established to be CGK by Professor Lawless.
340. Niemz went on:
‘Another laser treatment of the lens is the fragmentation of its interior rather than using ultrasonic exclusively [fn3: Laser fragmentation can significantly reduce the amount of necessary phaco time]. For this kind of treatment, picosecond laser pulses are advantageous, because they are associated with a lower threshold energy for the occurrence of optical breakdown if compared with nanosecond pulses. Thus more energy can be converted to the ionising process itself. In figure 4.8 the fragmentation of a human lens is shown which was obtained by using a picosecond Nd:YLF laser. The surgeon steadily moves the focus of the laser beam without injuring the capsule. During this treatment it is important to choose a pulse energy well above the threshold of optical breakdown because otherwise all laser energy will be absorbed by the retina and other tissues lying underneath.’
341. Although the second passage provides less information about the way in which the laser is controlled the suggestion is that it is under the manual control of the surgeon. It will be recalled that it is the central portion of the lens which is the most difficult to fragment and that the outer regions of the lens are more easily fragmented and removed so this procedure may not require precise control of where the laser is cutting, provided no further incisions are made in the remainder of the lens capsule. In any event, it was CGK for a surgeon to use dyes to visualise the position of the phaco tip in relation to the posterior capsule.
342. Additional detail as to how laser operation in the lens was controlled is contained in a 2004 paper by Ripken et al. entitled ‘Investigations for the correction of presbyopia by fs-laser induced cuts’. Although this paper itself is not CGK I am satisfied that the control of the laser inside the lens at least approximates to CGK, even if the precise details of the laser set-up might not have been. The paper describes experiments on eyes from two-year old pigs, using a femtosecond laser with a 5kHz repetition rate, 150fs pulse duration and up to 1.5W output power, and using energy of about 1 µJ . In the explanation of experimental methods the paper explains:
‘To create cuts inside the lens, the focus of the laser beam has to be scanned inside the lens tissue. Therefore the beam can be positioned by a two mirror galvano-scanner in the x-y plane with an operating range of nine millimetres in diameter and a resolution of better than one micron. To achieve a translation in the direction of propagation, a micro translation stage can change the distance between the scanner and the focusing optics on the one side and the fixation unit on the other by moving the treated eye or just the lens within a sub-micron resolution (figure 3). This fixation unit consists either of a glass plate that aplanates the cornea surface surrounded by a suction ring, that fits to the curvature of the treated eye or of a much smaller suction mask optimised in size for extracted pig lenses. The focusing optic is a f-theta-optic with a 75 mm focal length optimized for 780 nm wavelength and fs pulses. So, the laser can be focused to a minimal spot size of around 5 µm, as proved i.a. with a scanning knife-edge method. With this scanning and translation system it is possible to locate the focus and thus the optical breakdown region in any desired 3-dimensional pattern inside lens tissue with an accuracy of one micron.’
343. The description of the laser and this scanning unit is provided in the section on experimental methods, as a matter of routine. There is nothing to suggest that this description is anything out of the ordinary for the type of equipment which the Skilled Team would either have already or which they would be able to build. Hence why I consider it right to rely on this description as an indication of the way in which the Skilled Team would control a laser inside the lens.
344. Furthermore, although the Patents describe a number of scanning patterns to image the lens capsule, the lens cortex and the lens nucleus, as soon as the Skilled Team has decided to image those features, the decision as to which scanning pattern to try or use is trivial.
345. Ultimately, what I described as largely an absence of evidence as to what was CGK so far as control of lasers in ophthalmology procedures may not overly matter, for two reasons. First, because the Patents assume the Skilled Team can design and build a control system from their CGK. Second, because both pieces of prior art in this case teach (in different ways) methods of control, but make similar assumptions as the Patents that those skilled in the art can implement their teaching. However, where it may make a difference is as to the degree of interest which the Skilled Team would have in such teaching, so I may have to consider this further below.
346. For the pleaded validity attacks (obviousness and insufficiency) neither side contended that this case required anything other than the application of standard and well-known principles. Notwithstanding that, it is still useful to have the principles well in mind.
347. For obviousness, the correct legal approach is that summarised in Actavis v ICOS [2019] UKSC 15 at [52]-[73] per Lord Hodge, referring to the structured approach in Pozzoli v BDMO [2007] EWCA Civ 588 at [14]-[23] per Jacob LJ and citing Kitchin J. in his well-known passage from Generics v Lundbeck [2007] EWHC 1040 (Pat) at [74].
348. Since there are major issues on disclosure, I also mention the following passage from Philips v Asustek [2019] EWCA Civ 2230, per Floyd LJ at [61]:
‘The task for the party attacking the patent on the ground of obviousness is to show how the skilled person would arrive at the invention claimed from the disclosure of the prior art. If the invention claimed is, as it is here, a simple idea, then it is correct that this simple idea is the target for the obviousness attack. That does not mean, however, that the court is entitled to assume that the skilled person takes a different approach to the prior art, stripping out from it detail which the skilled person would otherwise have taken into account, or ignoring paths down which the skilled person would probably be led: see the passage from Pozzoli cited above. The nature of the invention claimed cannot logically impact on the way in which the skilled person approaches the prior art, given that the prior art is to be considered without the benefit of hindsight knowledge of the invention.’
349. The insufficiency squeeze in this case invokes ‘undue burden’ insufficiency.
350. Before I discuss the prior art, I mention two preliminary matters. First, Alcon’s preference was to examine Mühlhoff first because they considered that the stronger case. AMO urged me to consider Freedman first because they submitted it would demonstrate how the approach of Professors Lawless and Mrochen was tainted by hindsight. For that reason, I will consider Freedman first.
351. Second, I need to draw attention to the way in which AMO’s experts considered each piece of prior art.
352. Mr Benjamin rightly acknowledged that both Freedman and Mühlhoff contain considerable detail which is directed towards the SE. He indicated he would not comment on those details, instead focussing on what the SO would take from them, by which he meant his SO. His SO took a confined approach to what was disclosed.
353. The first two sections of the Technical Background section above covered the anatomy of the eye and an overview of cataract surgery. Professor Bouma took the view that neither formed part of the CGK of the SE. He indicated that his SE would have been aware that lasers and imaging systems were used in medical contexts, including ophthalmology, but his SE would not have had a detailed understanding of specific clinical applications of lasers or imaging systems, nor would he have been aware of the nature or clinical requirements of any clinical procedures, whether involving lasers and/or imaging or not. This approach meant that his SE did not pick up on the significance of some of the teaching.
354. Since the two men never had a discussion about any of their evidence, let alone about the prior art, their combined approach left, in my view, a significant gap between what each of them said was disclosed and what the proper Skilled Team would take from each piece of prior art. This enabled them (and AMO) simply to ignore teaching which the proper Skilled Team would have found significant and interesting. Examples will appear below.
355. This very restricted approach naturally impacted the evidence from each man as to what they considered was or was not obvious over each piece of prior art, which was doubly flawed because of their erroneous approach to the Skilled Team and their CGK. Again, examples will appear below.
356. Freedman is a US Patent entitled Laser Surgery Device and Method, filed in January 1995 but published in September 2002. AMO characterised Freedman as being all about RK. It is true that the specific embodiment in Freedman describes a system for performing RK using an ablating laser. However, the disclosure is wider than that. Therefore it is necessary to examine the disclosure with some care.
357. Under the heading ‘Background of the Invention’ Freedman says ‘This invention is directed to a laser surgery device and method controlled by interferometry.’ This is important. As will be seen, the key disclosure in Freedman is of a laser surgery system in which the treatment laser is controlled by OCT.
358. Under the next heading ‘Background’, I set out the first two paragraphs because they were the focus of attention in cross-examination due to the reference to the use of a laser in ‘clearing cataracts’. I return to consider the significance of this reference later:
‘Laser surgery methods include ophthalmic procedures, dental procedures and irradiation of tissue for hemostasis, photodynamic destruction of forms of tumors, removal of epidermal growths and abnormalities and for the ablation of atherosclerotic plaques. Lasers have been used in surgical procedures to cut tissue and to immediately coagulate the cut. Lasers have been used to control bleeding during surgical removal of burn wound eschar and in surgery on highly vascularized organs such as the liver.
Typically in laser surgery, heat generated by the laser is harnessed to destroy tissue. While thermal effects are commonly used in medical surgical methods, other nonthermal effects are utilized as well. Photons from laser beams can drive chemical reactions, break atomic bonds that hold molecules together or create shock waves to achieve various surgical objectives. Biomedical applications include such tasks as unclogging obstructed arteries, breaking up kidney stones, clearing cataracts and altering genetic material.’
359. In the third paragraph, Freedman turns to consider the problem his invention is trying to solve:
‘Most laser surgical methods utilize the laser heat effect. If the wavelength of light from the laser is matched very closely with the absorption band of the target structure, the laser light will be absorbed by, and therefore damage only that structure. The heat effect of the laser can be extremely selective and precisely controlled. However, in many surgical methods, it is difficult or impossible to choose an irradiating wavelength that will damage target tissue without affecting surrounding tissue. The absorption wavelength of target tissue may not be known or cannot be determined because of turbidity of tissue or other reasons. The absorption band of target tissue may not be distinguishable from the absorption wavelength of surrounding tissue.’
360. Freedman then refers to a prior US patent which proposed using ultrasonics to control laser surgery but explains its limitations, in particular for very small structures or smaller elements of larger structures. Accordingly, under ‘Summary of the Invention’ Freedman says:
‘The present invention relates to a method of laser surgery that permits detection and distinguishing of structures 10 microns in size and smaller permits detection and distinguishing of structures microns in size and smaller. The method permits control of laser surgery without requiring an intrusive probe. The method permits detection of tissue mass that is located within turbid tissue or within tissue having sonic characteristics that are identical to the characteristics of target tissue mass.
361. A laser treatment beam is controlled by interferometry, preferably by optical coherence tomography:
‘The method can comprise projecting an interference light beam onto a multilayer target of biological tissue, detecting the interference light beam reflected by the multilayer target to provide an interferogram, evaluating the multilayer target on the basis of the interferogram, and controlling the laser treating of the biological tissue according to the evaluating step.’
362. So interferometry is used in an evaluating step to create an interferogram (i.e. an image) of the tissue to be treated, which is then used to control the treatment laser.
363. Freedman contains five drawings and they are introduced at this point. Figs 1 and 3 are schematic representations of devices and methods for laser surgery controlled by low-coherence interferometry and Figs 2, 4 & 5 are ‘schematic representations of thin film layers of biological tissue such as thin film layers of a cornea’.
364. Freedman then turns to his description of preferred embodiments which starts with a lengthy section describing two methods of interferometry, the first being thin-film interferometry and the second OCT, followed by reference to four US patents describing interferometry devices, the disclosures of which are incorporated by reference. Freedman turns to a description of Figs 1 and 3, which show laser surgery devices using two-wavelength interferometry effectively to image a section of corneal tissue and to ‘determine displacement characteristics of an incision that is cut into the cornea tissue during radial keratotomy.’
365. Freedman describes RK as a very delicate procedure requiring precision. He explains:
‘The cornea is sensitive and delicate. The size and thickness of corneas vary from patient to patient. In performing a radial keratotomy, the length, width, depth and spacing of incisions must be precisely controlled in order to accomplish the desired object of improving vision without damaging the eye. The laser surgery devices 14, 64 and procedures illustrated in the Figures can control ablating of tissue to perform a radial keratotomy with high-intensity laser light by precise positioning of the laser beam and maximum absorption of the beam over a precise area and depth of incision.’
366. In the next paragraph Freedman makes clear that the description is not limited to RK (emphasis added):
‘According to the present invention, a sequence of detection can be used to evaluate the thickness and the boundary state of each layer of the cornea or other biological tissue. The cornea can be considered either a single layer or multilayer thin film. The cornea can be evaluated as a multilayer thin film to provide detailed information about cross-sectional planes of the cornea tissue or evaluated as a single layer thin film for applications requiring only gross information on the tissue structure. According to the invention, the information from the evaluation of the cornea has been found to be sufficient for processing to control the delicate ablation in a radial keratotomy and in other procedures for treating biological tissue by laser surgery.
367. In the detailed description of figure 1, the interferometer and optical system are used to create a ‘spatialgram’ which is then used to create an ‘ablating plan’ for an ablating laser:
Ablating laser device 52 includes laser generator 54 and laser beam irradiator 56 for applying a laser beam from the laser generator 54 as ablating beam 58 to an ablating target region 60 of the cornea 12 to form an incision. The ablating laser device 52 can include any device known in the art for conducting a radial keratotomy as for example devices disclosed in U.S. Pat. No. 4,648,400 to Schneider et al and U.S. Pat. No. 5,284,477 to Hanna et al. The device 52 includes an emitter for emitting a pulsed laser beam. The beam can comprise one lobe of elongated cross-section. A focussing means of irradiator 56 can focus the image of the lobe or lobes of the laser beam 58 onto the region 60 of the cornea 12 to be corrected. A displacement means 62 displaces ablating light beam 58 across the cornea 12 while focussing the lobe or lobes of beam 58 to complete correction of the cornea 12 as the summation of a plurality of elementary discrete ablations.
368. Alternatively, the ablating plan can be constructed with input from the surgeon.
369. There is also a detailed description of Figs 3-5, followed by a description of using low-coherence tomography in several OCT sequences to three dimensionally image a target cornea and to precisely incise the cornea with a laser. Various modes of controlling the laser are described. For example, in column 8:
‘In another procedure, an absolute distance to the target of biological tissue (for example the distance between the ablating laser 52 and the surface of the cornea 12 can be determined by the procedure described with reference to Figs 3 and 4.’
370. This is done by evaluating a phase difference between a reference beam and a measurement beam. Further down in column 8, Freedman describes further details of methods of control. First, ‘real-time’ control and then ‘concurrent’ control:
‘The processor 48 can be a computer that determines the location and size of tumours or of cornea tissue and incisions and ablation using the information from the interferometer of figure one or figure three or a combination. Based on such information the computer can determine the total power intensity, pulse duration and repetition rate and position of a light guide for irradiation laser 56 the computer can provide real time information graphic representation of structures such as a cornea along with information relating to the progress of ablation such as information on tissue destroyed or incised.’
‘In another embodiment, ablation is concurrently controlled by detecting the extent of incision. Cornea ablation by ablating beam 58 is controlled by detecting the extent of the incision with the interference beam during ablation and simultaneously controlling ablating beam 58. The power intensity, pulse duration and repetition rate and focus of the beam 58 can be concurrently adjusted according to a comparison with the incisions previously determined by the surgical model of the ablating plan. The cornea ablation can be controlled by using the ablating beam 58 by intermittently emitting a measuring pulse that determines the extent of incision and compares the extent to the surgical model. The power intensity, pulse duration and repetition rate and focus of the beam 58 can be controlled from the comparison.’
371. Professor Mrochen said (and I accept) that what the SE would understand from this second passage was an automated process for control of corneal ablation by detecting the extent of ablation and simultaneously controlling the ablating beam accordingly (including parameters such as the power intensity, pulse duration, repetition rate and focus of the beam).
372. The specification concludes with a paragraph which begins:
Other modifications of the present invention will occur to those skilled in the art subsequent to a review of the present application. For example, the device of FIG. 1 can be modified to determine an image of a cornea or other optically transmissive tissue by sequentially determining thickness by coherence shifting interferometry wherein the system utilizes an optical energy source for generating a source beam.
373. This modified version of Fig 1 comprises a ‘Mach-Sehnder’ type interferometer, in which the amount of adjustment in the variable optical path length ‘provides a measure of the unknown thickness that can be analysed by a processor for control of an ablating laser.’
374. In cross-examination, Professor Mrochen agreed that this passage proposes a variation to the Figure 1 device which operates by thin-film interferometry; that the variation was aimed at the same goal, which is measuring the thickness of the cornea by thin-film interferometry using light reflected from the front and back surfaces of the cornea, and then using that thickness in the control of an ablating laser; that thin-film interferometry is only used for imaging structures that are composed of thin films and that it would not apply to the lens.
375. This creates something of a conundrum. Other than the cornea, it is difficult to identify any ‘other optically transmissive tissue’ to image for the purposes of treatment other than the lens - and at the very least the lens must be the prime candidate indicated by this expression. Yet the evidence was that thin-film interferometry did not apply to the lens. One possibility was that thin-film interferometry might be applicable to the lens capsule, but there was no evidence given to that effect so I set that consideration aside.
376. Those points having been established, Professor Mrochen was challenged why he had relied so heavily in his reports on this reference to ‘other optically transmissive tissue’. His answers showed, in my view, that he was prepared to take this expression out of its context and to use it to reinforce his conclusion on obviousness.
377. Freedman contains a number of claims. Whilst there are numerous subsidiary claims specific to RK, there are also general claims which reflect some of the earlier general disclosures (i.e. consistory clauses) under the heading ‘Summary of the Invention’.
378. When discussing what Freedman disclosed, Professor Bouma, in his first report, confined his discussion to the two embodiments in Figs 1 and 3. So his focus was immediately on RK and no other application. Professor Bouma was of the view that the reader of Freedman would find and read the Schneider and Hanna patents and find, as he did, that they disclosed using an excimer laser of various wavelengths. Mr Benjamin’s approach was not quite so precipitate, but his first report also ignored the more general teaching, describing the focus of Freedman being ‘on a laser device which can perform RK’. His view was that his SO would not have been motivated to pursue Freedman because RK had all but been abandoned in favour of PRK, ALK, LASIK and LASEK. Again, he paid no regard at all to the more general teaching in Freedman, and he had ignored the fact that RK was still in use to treat astigmatism.
379. In their second reports, Professor Bouma and Mr Benjamin responded to the more complete discussions of the disclosure in Freedman in the first reports of Professors Mrochen and Lawless. Professor Bouma dismissed the reference to ‘clearing cataracts’ stating his view that the SE would not read Freedman as suggesting use of his device in ‘clearing cataracts’, emphasising that it would not have been possible to do so, ‘as the device is only suitable for treating the surface of the cornea’. So Professor Bouma saw Freedman as limited to surface treatment of the cornea using an ablating laser (specifically a UV excimer laser). He dismissed Professor Mrochen’s suggestion that the Skilled Team might use a femtosecond laser.
380. Similarly, Mr Benjamin dismissed any attempt to characterise the teaching of Freedman as going beyond RK using an ablating laser. He characterised the reference to ‘clearing cataracts’ as simply part of a general introduction to the previous surgical uses of lasers, and the SO would think, if he paused to think about it, that it was a reference to the Dodick Nd:YAG laser (then recently demonstrated in 1991) to break up the lens nucleus using shockwaves.
381. In my view, both Professor Bouma and Mr Benjamin took too narrow view of the disclosure of Freedman. It is true that the specific embodiments are directed to RK and the use of an ablating laser, but the disclosure is of a laser surgery device controlled by interferometry and preferably OCT, ‘to control the delicate ablation in a radial keratotomy and in other procedures for treating biological tissue by laser surgery’.
382. Freedman contains a rather general description of RK (col 4, lines 14-32). It contains very little disclosure of suitable lasers. Undoubtedly, in my view, the main thrust of the teaching is using interferometry to create an image of the tissue to be treated and to control a laser surgery device. Although Freedman promises the ability to detect tissue mass that is located within turbid tissue, the Skilled Team would understand that a natural application was the eye, precisely because it contains significant non-turbid tissue. The skilled reader would suspect that Freedman chose RK as an example to illustrate the degree of precision which interferometry and OCT in particular would provide to laser surgery. Indeed, Professor Lawless said that the SO would have been very interested in the potential of the method and devices described in Freedman, given the difficulty of and precision required in the performance of RK. The Professor’s point was confirmed by some evidence from Mr Benjamin that the precision taught in Freedman for RK was greater than that required for AC or LF.
383. In terms of the levels of precision which Freedman teaches the skilled reader, in addition to the promise of the ability to detect and distinguish structures of 10 microns in size or smaller, there is the more concrete promise of being able to evaluate the thickness and boundary state of each layer of the cornea (or other biological tissue) and also the ability to control the position and intensity of the laser during treatment to ensure the incision is as planned.
384. When considering the evidence I received relating to Freedman, there are two general points:
i) First, as I mentioned above, neither Mr Benjamin nor Professor Bouma treated the disclosure of Freedman fairly. Both took too narrow view of its disclosure. Neither read the document with the interest with which the Skilled Team would bring to their consideration of Freedman. For that reason alone, I discount the views they expressed in their written evidence about what was obvious for the Skilled Team to do having read Freedman.
ii) Second, the cross-examination of Professors Mrochen and Lawless on Freedman was clearly inspired by the rather narrow and literal views which Mr Benjamin and Professor Bouma took of Freedman. On that basis, the principal challenge was that significant hindsight was required to find any inspiration or motivation to take the ablating RK laser device of Freedman forward and similarly, that the focus on ‘clearing cataracts’ was again inspired by hindsight.
385. I accept that the degree of motivation for the Skilled Team to take Freedman forward depends on a number of factors, including the length of time since Freedman was written; the Skilled Team’s view of RK and the Skilled Team’s CGK as to how both lasers and OCT had progressed since Freedman was written. However, I find the Skilled Team would have taken interest in Freedman’s teaching, when considered with their CGK. Where that would have led them is the next topic.
386. In terms of the differences between Freedman and the principal claims of the Patents, the parties were agreed there were two. Freedman does not teach:
i) The use of his system to perform AC or LF.
ii) A laser which can effect photodisruption.
387. Alcon submitted that if the Skilled Team decides to take the first step, the second one follows. AMO submitted that the obviousness case required the Skilled Team to take two mental leaps simultaneously.
388. In closing, Alcon put their case on the basis of the general disclosure of Freedman. In other words, having read and considered the whole document with interest, the Skilled Team would reason as follows:
i) They would not be particularly interested in the specific embodiment because RK was not used anymore, except for treating astigmatism.
ii) Nonetheless, the Skilled Team would be interested in the promise of the more general teaching in Freedman of using OCT to create an image of the tissue to be treated and to control a laser surgery device to make incisions in that tissue.
iii) The Skilled Team would know that the capabilities of lasers and OCT had improved significantly since Freedman was written and would apply his teaching in the context of their CGK of lasers and OCT i.e. that the OCT system could create a suitably precise image of the lens capsule and lens and a precisely guided femtosecond laser would be able to create incisions using a high number of comparatively much smaller photodisruptive bubbles than used in previous attempts, generating far less heat in the tissue.
iv) The Skilled Team would recognise that Freedman’s general teaching could be applied to various types of tissue in the eye, but the mention of ‘clearing cataracts’ would put them in mind of applying this teaching both to create an incision in the capsule (both anterior and posterior) and to fragment the lens. (In this regard, it is relevant to note that Mr Benjamin considered the precision taught in Freedman for RK was greater than that required for AC or LF, but he also recognised that an improvement in precision is of benefit in any application).
389. This is a case which has some force because of the consequence of Freedman’s teaching which makes an explicit link in the minds and discussions of the Skilled Team between their CGK femtosecond laser and its control using their CGK OCT. ‘Control’ in this sense comprises creating an image of the tissue to be treated and then guiding the laser with a high degree of precision. The Skilled Team would also recognise that ‘precision’ had two aspects. The OCT system was able to image and guide the laser with a high degree of precision, but the incision created by the laser pulses would be extremely precise, because the incision is created by a high number of smaller photodisruptive bubbles, likely to generate far less heat in the tissue. I also point out that if the Skilled Team would not have been able to build an OCT device which could create a suitably precise image of the lens capsule and lens, the Patents would be insufficient.
390. Against this, AMO and their experts put a considerable number of reasons why they contended it would not have been obvious to apply Freedman to create an AC or LF system.
i) First, no motivation to improve existing techniques, but I have decided that point against AMO.
ii) Second, Freedman only disclosed the use of a UV ablating laser to perform RK. This is the illustrated embodiment, but the point ignores the more general teaching.
iii) Third, the Skilled Team was required to take two mental leaps simultaneously, but I consider that AMO exaggerated the step of changing the laser from ablative to photodisruptive. Furthermore, the Skilled Team would not have in mind a 1995 photoablative laser but the capabilities of lasers available to them at the priority date. The Skilled Team would select a laser suitable for the application they had in mind i.e. not a UV excimer laser but a photodisruptive laser in the infrared range. So, in a very real sense, the second step would automatically follow the first, if it was made.
iv) Fourth and by far AMO’s biggest point was that both steps (and the first in particular) could only be made with hindsight.
391. The foundation for AMO’s hindsight point had a number of elements. I deal with the principal points individually and then assess the cumulative result:
i) First, the mention of ‘clearing cataracts’ was said to be properly confined in the mind of the Skilled Team to a historical reference to the Dodick system. I do not consider such confinement to be warranted.
ii) Second, that the reference to imaging ‘a cornea or other optically transmissive tissue’ would not be seen as ‘somehow suggesting use of the device to image a lens’ as Professor Bouma said, because this phrase is used in the context of thin-film interferometry which Professor Mrochen agreed was not applicable to the lens. I have discussed this conundrum above. I agree that both Professor Mrochen and Lawless took this reference out of context and generalised it beyond that context. Professor Lawless for example, seems to have understood this teaching to be ‘accurate three-dimensional imaging of ‘a cornea or other optically transmissive tissue’’, which is incorrect.
iii) Third, confining the disclosure of Freedman to the use of an ablative laser, guided by OCT, for the purpose of RK. This ignores the more general teaching in Freedman.
iv) Fourth, criticism of Professor Mrochen’s evidence that the Skilled Team reading Freedman would have considered a pulsed femtosecond laser to be a ‘good fit for procedures requiring precision and accuracy’. AMO submitted that Professor Mrochen was simply wrong about the disclosure of Freedman, but Professor Mrochen did not actually say that Freedman disclosed photodisruption. Rather the point he made in his second report was that the Skilled Team would not understand the teaching to be limited to an excimer laser in the UV or VUV range but to use a laser appropriate to the application.
v) Fifth, criticism of Professor Lawless who stated that integer (b) of EP861 was disclosed in Freedman i.e. that Freedman disclosed a laser effecting dielectric breakdown i.e. photodisruption. When this was pointed out to him in cross-examination, Professor Lawless readily acknowledged his mistake and apologised.
392. Standing back from the detail, this issue is reasonably finely balanced (and much closer than AMO would have it). Freedman puts into the mind of the Skilled Team the link between the laser and controlling it using an OCT system and the general teaching does hint at applications beyond the cornea. However, on balance, I am left with the impression that Professors Mrochen and Lawless were trying too hard to get from Freedman to within the principal claims of the Patents, in other words that their reasoning was tainted by hindsight, principally on the second and fifth points above. For this reason, I must find that the principal claims of EP861 and EP528 were not obvious over Freedman.
393. Before one gets to consider the obviousness attack over Mühlhoff, it is necessary to resolve some key disputes over what Mühlhoff disclosed to the Skilled Team. These issues concerned in particular:
i) The relationship between the 5th embodiment and the first four. This turns largely on a sentence in [0158], but also on more general considerations.
ii) The significance of the teaching in [0015].
iii) The teaching of the 5th embodiment including whether it was limited to the use of multiphoton fluorescence (MPF) and the significance of ‘laser-induced tissue-specific signals’.
394. It is with those disputes in mind that I turn to consider what Mühlhoff disclosed to the Skilled Team.
395. Mühlhoff is a PCT application filed by Carl Zeiss Meditec AG on 22 August 2003 and published on 1 April 2004. It is entitled ‘Device and Method for Measuring an Optical Penetration in a Tissue’. The document is in German and I was provided with a translation. One of the difficulties in translating this type of technical document is that an accurate translation requires an understanding of the technology, which the translator may not have. In the original, the word translated as ‘Penetration’ in the title (and also in the Abstract) is Durchbruchs which literally means breakthrough but in the translated specification is translated as ‘breakdown’. Fortunately, the specification explains what is meant.
396. [0001] says the invention ‘relates to an apparatus for measuring an optical breakdown triggered in a tissue below a tissue surface by treatment laser radiation.’. [0002] explains that the treatment laser radiation acts by photodisruption or photoablation. [0003] explains that if the power density of the radiation exceeds a particular threshold there is an optical breakdown which generates a plasma bubble in the tissue. It also explains why Mühlhoff regards photoablation and photodisruption together. It is evident that Mühlhoff ascribes the same mechanism of action to both - the application of sufficient power intensity at a position creating a plasma bubble. Mühlhoff explains:
‘If a plasma is generated at a tissue interface, which could also be located within a tissue structure by all means, there is tissue ablation from the interface. Therefore, this is then referred to as photoablation. The case where a plasma bubble separates previously connected tissue layers is usually referred to as photodisruption. For the sake of simplicity, all such processes are subsumed here by the term optical breakdown, i.e. this term includes not only the actual optical breakdown but also the effects in the tissue resulting therefrom.’
397. [0004] explains that significant focussing of the laser beam in conjunction with very short pulses allows the very precise use of the optical breakdown in a tissue. [0005] says that in recent times, the use of pulsed treatment laser radiation has prevailed, particularly for laser-surgical refractive error correction in ophthalmology. In [0006]-[0008] Mühlhoff acknowledges four prior art patents, including a method for refractive error correction by isolating a lenticular partial volume in the cornea and removing it by means of an incision to one side, with the form of the partial volume being designed to bring about the desired refractive error correction.
398. [0009] makes the point that accuracy has a direct effect on the quality of the result. Thus, the object of Mühlhoff is to develop an apparatus (and method) for measuring an optical breakdown in order to increase the accuracy of the effect of a treatment laser radiation.
399. Having stated the object of the invention, there are some important paragraphs of general teaching before Mühlhoff starts to describe his five preferred embodiments.
400. Mühlhoff achieves this object by detecting the spatial extent and/or relative position of the optical breakdown in the tissue by detecting radiation emanating from the tissue itself, where ‘emanating’ means backscattered, reflected or induced radiation, as opposed to transmitted. Mühlhoff also explains in [0011]:
The method … and the apparatus according to the invention are suitable, in particular for measurements in treatment of transparent or semitransparent tissue, since up to three-dimensional structure information can be obtained in this case. Hence the invention is particularly well suited to the monitoring of microsurgical operations on the eye.
401. [0012] explains that the detection signal can be used to control the treatment radiation in various ways: by controlling laser parameters including beam cross-section, intensity and/or pulse duration, and the control can be manual, semi-automatic or fully automatic by closed-loop control. Control of laser parameters can also include shaping the beam and deflection parameters which control its location i.e. relative position of the optical breakdown in the tissue, again facilitated by the use of a control loop.
402. [0013] explains the advantages of closed-loop control over what it says was the prior art position of sensing the treatment laser radiation parameters prior to treatment, a process which Mühlhoff describes as very much more indirect because the interaction with the tissue remains unaccounted for. By contrast, detecting radiation from the tissue allows a very much more accurate closed-loop control of the treatment laser radiation since the optical breakdown is captured directly.
403. It is clear from the first sentence of [0014] that Mühlhoff is considering femtosecond lasers. The third sentence hints at the use of MPF which emerges later in the fifth embodiment:
‘Ultrashort laser pulses in the infrared or visible spectral range (400 to 1900 nm) with pulse durations ranging between 1fs and 100 ps are particularly preferred for the treatment laser radiation. This optical radiation can penetrate tissue, particularly the transparent parts of the eye (cornea, lens, vitreous humor). In the case of high power densities, which are only achieved at the focal point, the laser pulses trigger nonlinear optical processes in the form of optical breakdowns, as may be caused by multiphoton excitation or frequency conversion, for example, where in the required power density may be tissue specific.
404. There then follows [0015], the first part of which was a particular battleground at trial. That part reads as follows:
[0015] The invention is particularly suitable for the aforementioned operating procedure provided for a refractive error correction. In addition, the invention could also be used for other ophthalmological or other surgical interventions. These include incisions for refractive eye surgery or for removing enclosed foreign bodies, incisions in the cornea, incisions in the vitreous humor of the eye, in the lens or in the sclera. Likewise, localized laser-induced tissue changes without incision effects are also conceivable; these could reduce opacification or hardening of the cornea. However, other tissues are also transparent to infrared radiation, for example the dermis.
405. The document then goes on to describe its five embodiments twice, the second time in more detail than the first. It is important to keep this in mind, because the first disclosure of each embodiment contains more general teaching whereas the second disclosure is more detailed and specific. Here I give a brief description of each embodiment and the references:
i) The first embodiment, described in [0020]-[0030], [0082]-[0112] & Figs 1-8, is a system in which interferometry, preferably an OCT device, is used to detect radiation emanating from the tissue.
ii) The second embodiment, described in [0030]-[0035], [0113]-[0124] & Fig 9, is a system in which confocal microscopy imaging is used in place of the OCT device, as is the third embodiment, described in: [0036]-[0043], [0125]-[0133] & Figs 10-13.
iii) The fourth embodiment, described in [0044]-[0050], [0134]-[0148] & Figs 14-18, is a system that uses a slit lamp optical unit.
iv) The fifth embodiment, described in [0051]-[0059], [0149]-[0160] & Figs 19-22, is a method in which the tissue is both diagnosed and measured in three dimensions and also treated where the tissue is earmarked for treatment.
v) In this fifth embodiment, Mühlhoff discloses that it is preferable for the treatment laser also to act as the measurement beam. This provides a common reference point, so that a tolerance chain, which may arise when using separate systems, is avoided. An energy reducer can be employed to reduce the power of the treatment laser radiation so it can be used for measurement. This embodiment also allows a second treatment step to be applied e.g. if the sparing application of the laser treatment beam has not quite achieved the object of the treatment.
406. Having introduced each embodiment with general teaching, at [0060] the specification turns to list the figures in the usual way and then describes, in [0082]-[0089], a particular example operating method by reference to Figures 1 and 2.
407. The laser surgical system generates a pulsed treatment beam with a pulse duration in the nanosecond or femtosecond range. This is used to correct a refractive error by removal of material from the stroma within the cornea. By focussing the treatment laser at points within the stroma, plasma bubbles are created and when a series of them are strung together, the treatment beam ‘acts like a surgical knife which, without injuring the surface of the cornea, directly cuts material in the interior of the stroma.’ [0085]. A partial volume inside the stroma is cut and the laser incision is then continued to the surface of the cornea whereby the isolated material can be removed laterally. The incision is made ‘in accordance with parameters ascertained in advance’ [0086]. [0088] explains that the smaller the plasma bubbles, the finer the incision generated by the laser-surgical instrument.
408. A measuring apparatus is provided for monitoring the precise incision, capturing the spatial extent and/or relative position of the plasma bubbles. It can also be used to control and optimise the scanning movement of the treatment beam and the beam parameters to ensure the required diameter and position of plasma bubbles to create the required incision. Optimisation allows the plasma bubbles to be kept as small as possible and the incision as fine as possible. It is emphasised in [0088] that the precision and fineness of the cut is particularly important at the edge of the lenticular partial volumes in this particular treatment.
409. By reference to Fig 2, [0090] then turns to the first embodiment in which the measuring apparatus is an OCT device. It is said to follow the principle described in the Izatt paper, with the reference given. If the Skilled Team were not already aware of this paper, they would refer to it, and find this image (amongst others, taken using a slow experimental system in 1994 or earlier) showing the location of the anterior and posterior capsule in a bovine eye:
410. Figure 2 shows the use of a PC to read the signals from the OCT device so that ‘the surgical instrument operates with online monitoring and online closed-loop control’ [0104]. Mühlhoff describes a time domain OCT device, but also explains how to achieve better axial resolution. [0098] explains that the measurement beam can be focused to different depths within the tissue. [0099] goes on to explain how relatively tight focusing of the OCT beam will improve the resolution. The Skilled Team would recognise this as teaching OCM (see paragraph 131 above). The axial resolution is indicated as being in the order of 10µm.
411. Figure 5 (described in [0106]) is a schematic illustration of the incision carried out under online monitoring.
412. A ‘lenslet’ 15 is cut from the stroma by a multiplicity of plasma bubbles 11. [0107] explains that after the incision to form the lenslet, a lateral incision 16 is carried out which allows the lenslet to be removed in the direction 17, the incision situate at the optically less important edge of the cornea 14.
413. The remainder and the bulk of the specification is concerned with the various types of measuring apparatus that have already been introduced.
414. It is not necessary for me to rehearse all of the detailed teaching in Mühlhoff about each of the five embodiments, but it is necessary to deal with the fifth embodiment in particular.
The fifth embodiment
415. In the first set of paragraphs relating to the fifth embodiment, there is no mention of multiphoton fluorescence. Instead, Mühlhoff discloses what the imaging system does. In particular, tissue specific signals are identified as the means by which relative positions of interfaces and/or inclusions in the tissue are identified. [0051] describes the method for diagnosing, measuring and treating transparent or semi-transparent tissue:
[0051] The fifth embodiment of the invention allows the tissue to be both diagnosed and measured in three dimensions and also be treated where the tissue is earmarked for treatment. To this end, the following is provided: a method for measuring a transparent or semitransparent tissue, wherein illumination laser radiation is focused at a focal point in the tissue and the relative position of the focal point in the tissue is altered, for the purposes of which a changeable deflection of the illumination laser radiation is undertaken, and wherein tissue-specific signals induced by the focusing are detected and assigned to measurement points, the location of which in the tissue is defined by the determined relative position of the focal point in each case, and wherein measurement points are filtered out and, as a result thereof, relative positions of interfaces and/or inclusions in the tissue are determined.
416. This passage is important in view of the argument over whether the fifth embodiment necessarily entails the generation of tissue-specific signals (TSS). What [0051] explains is that the whole point of TSS is to detect the relative positions of interfaces and/or inclusions in the tissue. I doubt that the expression ‘tissue-specific signals’ should be interpreted as literally as was implied in some of the evidence from Professor Bouma. He seemed to think the system would be able to detect a signal and indicate it was from e.g. the stroma or the epithelium automatically. It is far more likely, in my view, that the Skilled Team would understand the system depended on detecting where differences between signals occurred. The locations where these differences occurred, together with knowledge of the basic structure of the eye, would indicate the positions of interfaces and/or inclusions in the tissue.
417. To similar effect [0052] describes the apparatus:
[0052] This method can be realized particularly advantageously using an apparatus for measuring a transparent or semi- transparent tissue, comprising a laser radiation source, a deflection device, a focusing device and a detector device and also a control device, the latter driving the laser radiation source, the deflection device and the focusing device in such a way that illumination laser radiation emitted by the laser radiation source is successively focused on a plurality of focal points within the tissue by means of the deflection device and the focusing device, wherein the detector device emits tissue-specific signals, induced by the focusing, to the control device and the control device assigns the signals to measurement points, the location of which in the tissue is determined in each case by the relative position of the focal point, and filters out measurement points and thereby determines the relative positions of interfaces and/or inclusions in the tissue. (emphasis added)
418. This teaching (and other passages to like effect) makes it clear that particular tissue in the eye is not (necessarily) identified by a signal which is uniquely ascribed to a particular tissue type but by identifying the interfaces between different types of tissue in the eye, combined with the knowledge of the usual make-up of different tissue structures in the eye.
419. [0055] explains it is preferable for the same laser to be used for both measurement and treatment, being guided by the same deflection device and the same focusing device, but with reduced power for measurement. In this way, all measurement and treatment points have a common reference and the tolerance chain is precluded. This means, as Professor Bouma accepted, that the earlier description of the fifth embodiment also included apparatus where different light sources were used for measurement and treatment even though the preference is for a single source.
420. [0058] indicates the degree of accuracy which can be obtained:
[0058] The signals detected in the detection beam path are assigned to measurement points which are each determined by the specific position of the detection beam path, for example by the specific position of a focusing device and/or a deflection device. These signals can be stored in a memory and can be compared in a downstream comparator to a threshold which can be selected so as to be unchanging or so as to depend on the relative position of the individual measurement points. As a result, it is possible to determine all measurement points earmarked for a treatment. The corresponding relative position information is transmitted to a control device which sets an appropriate sequence for the generation of optical breakdowns. The treatment laser radiation is then moved along an appropriate trajectory with its focus. This can effectively prevent injury to tissue that should not be processed, even if a point to be treated is located very close to tissue parts that should remain uninjured. The obtainable accuracy is of the order of the focal diameter and can be even below 1 µm, depending on focusing and radiation wavelength. Then, the energy reduction is terminated for the purposes of generating the optical breakdowns.
421. Thus, it seems to me that [0058] contemplates both unique tissue-specific signals and those determined by reference to interfaces.
422. The more detailed description of the fifth embodiment runs from [0149]-[0160]. A schematic is shown in Fig 19, which I need to set out:
423. The laser surgical instrument shown schematically in Fig 19 comprises the following parts: 71 is the pulsed laser beam source; 72 is the deflection device; 73 is a tuneable focusing device; 74 is an (optional) positioning device for positioning the tissue to be treated (identified in the text as 6, but clearly in Fig 19 it is denoted as 76); 75 is a control device for driving 71, 72 and 73 so that the focus of the laser radiation is focussed at real targets ZP’ with coordinates x’’’, y’’’ and z’’’. 77 is a removable energy reducer, 78 is identified in the text as ‘a detector’, 79 is a memory unit and 80 is the laser beam.
424. The second half of [0150] and [0151] explain that:
‘As a measurement beam, the laser beam 80 brings about a laser-induced signal S at the real measurement point MP depending on the properties of the tissue, said signal being received by a detector 78 via the detection beam path (not illustrated in any more detail). The detected laser radiation-induced signals S are fed from the output of the detector 78 to the input of a memory unit 79 and stored in the memory unit 79 together with the coordinates (x', y', z') of the captured associated measurement points MP'. In a comparator unit 81 connected to the output of the memory unit 79, the laser radiation-induced signals S are compared to thresholds  stored there.
stored there.
[0151] As a result, this selects the measurement points that should be impinged by the treatment laser beam as targets once the energy reducer 7 has been removed. As a result, the treatment regime is determined. The coordinates of these selected captured measurement points MP' are transmitted to the control device 75 and are available for driving the deflection device 72 and the focusing device 73.’
425. It is apparent from this description that the box marked 3 in Fig 19 is mislabelled and should be marked 78.
426. As would be apparent to the Skilled Team, [0152] explains that the measurement and target systems share the same coordinate system.
427. [0153]-[0157] then describe a series of measurement regimes by reference to Figs 20-22. These figures (and the accompanying text) show that with knowledge of the structure of the tissues in the cornea, one can reduce the number of measurement points which need to be taken for a given accuracy of measurement. The description makes clear that Mühlhoff is talking about the use of the imaging system to measure the relative position of interfaces between different types of tissue and/or inclusions.
428. The specification concludes with three paragraphs which I will set out because [0158] (and the last sentence in particular, which I have underlined) was the focus of a number of disputes:
[0158] The portrayed embodiments can be used particularly advantageously for the operating method mentioned at the outset. To this end, it is possible to measure the cornea of the eye, held against a contact glass by suction, with a high depth resolution (approximately 1 µm) and low lateral resolution (e.g., 100 µm) from the epithelium to the endothelium over the entire region, in which the surgical invention should be implemented. In the fifth embodiment, the energy reducer 77 is activated to this end, and the layers of the cornea are scanned in a manner substantially perpendicular to the corneal surface at a plurality of positions over a lateral 100 µm grid. In the detection beam path, a multiphoton fluorescence at a suitable wavelength, for example, which is sensitive to differences in the different layers and/or interfaces, is detected with a spatial resolution. Alternatively, any of the above-described measurement principles can be used.
[0159] Then, a three-dimensional image representation of the layer of the cornea can be created from a multiplicity of depth profiles obtained thus. In this image representation, it is possible to identify the laterally resolved relative depth position of Bowman's membrane, which may be of importance depending on the incision. For the treatment, the energy reducer is removed from the beam path such that, when the scanning procedure is carried out again, the desired incision is carried out below the epithelial boundary. As a result, the epithelium remains largely uninjured such that the incision has healed again after few days.
[0160] However, not only can the epithelium be detached along Bowman' s membrane, an incision lying deeper in the stroma is also possible. The thickness of the stroma remaining on the epithelium can be set precisely by the preceding measurement, as a result of which a damage to, or loss of, the epithelium is precluded.
429. Thus, ‘a three-dimensional image representation of the layer of the cornea’ is obtained. Once the imaging is complete, then for the treatment the energy reducer is removed and the desired incision is made below the epithelial boundary. [0160] then explains that not only can the epithelium be detached along Bowman’s membrane, an incision lying deeper in the stroma is also possible. Damage to the epithelium is precluded due to the precision of the imaging measurements.
430. Several issues arise on the way in which the experts said the skilled person would read Mühlhoff. Since neither side emerges unscathed from these issues, it is necessary to deal with them carefully and then assess the end result.
431. The first issue is as to the significance of [0015].
432. The second issue is rather involved and concerns AMO’s attempt to separate the fifth embodiment from the first four. AMO submitted that Mühlhoff disclosed two distinct types of system embodying two distinct concepts, as follows:
i) That in the first four embodiments, Mühlhoff disclosed systems in which the size and location of the plasma bubble in the cornea are determined as it is being created by the treatment laser, and the information generated is used to feed back into the control of the treatment laser to improve accuracy. These systems use separate OCT, CFM or slit lamp devices to determine the size and location of the plasma bubble.
ii) A system in which tissue-specific signals are generated to create a map of the cornea which is then used to plan the refractive surgery. This system requires a single laser source, and a common set of optics, to be used for measurement and treatment to ensure accuracy. The only suggested method of generating the tissue-specific signals is multi-photon fluorescence. This is the fifth embodiment.
433. The purpose of this submission was plain. On the basis of this sharp distinction, AMO contended that there was no disclosure of OCT with pre-planning and no disclosure that OCT would work in the fifth embodiment. For a series of reasons which follow, I am entirely satisfied that the Skilled Team reading Mühlhoff at the Priority Date would not perceive this sharp distinction between embodiments 1-4 and 5. To the contrary, since Mühlhoff in fact expressly teaches that OCT or any of the other imaging techniques can be used in the fifth embodiment set-up.
434. However, AMO’s supposed distinction in fact rests on a series of sub-issues which tended to get mixed up to varying degrees in cross-examination.
435. It is convenient to deal with all these issues and sub-issues in the following order:
i) What the Skilled Team would take from [0015].
ii) Whether the final sentence of [0158] referred to the four imaging techniques (to use a neutral word) the subject of the first to fourth embodiments or, as Professor Bouma contended, the measurement regimes illustrated in Figs 20-22.
iii) Whether the fifth embodiment is only concerned with ‘tissue-specific signals’ (TSS) or whether imaging which detects the boundaries between different layers of tissue is also sufficient.
iv) Whether the fifth embodiment is restricted to a system where a single light source is used for both measurement and treatment or whether different light sources can be used for measurement and treatment.
v) Whether the fifth embodiment is incompatible with OCT.
vi) Professor Mrochen’s insistence that the detector labelled 3 in Fig 19 was an OCT device, and various other criticisms made by AMO of Professor Mrochen’s evidence on this aspect of Mühlhoff.
vii) Whether the idea of imaging in advance of treatment (i.e. planning where to cut) is only disclosed in the fifth embodiment.
436. [0015]: In his first report, Professor Bouma examined Mühlhoff in some detail in his paragraphs 113-187, making reference to virtually every paragraph. He drew particular attention to the description of Fig 1 in [0082]-[0089], which I have discussed above, yet omitted reference to [0086]. Any discussion of [0014] and [0015] is also conspicuous by its absence, notwithstanding their clear teaching. In his second report, Professor Bouma said the SE would read [0014] and [0015] ‘as the kind of hyperbolic statement that inventors typically make in the introduction section of patent documents to describe the broad utility that their invention ‘might’ have.’ In that way, Professor Bouma rejected the teaching of those paragraphs out of hand.
437. It is clear, and I find, that neither paragraph would be read by the Skilled Team as hyperbole. For a start, the information in the first sentence of [0014] reflected the CGK. When cross-examined about his evidence in relation to [0015], Professor Bouma’s response was to say that he did not have the expertise to give evidence as to the suitability of devices for ophthalmic applications, an answer which confirmed his lack of competence to assert that the statements in those paragraphs of Mühlhoff were hyperbole.
438. For his part, Mr Benjamin noted that [0015] stated that ‘the invention could also be used for other ophthalmological or other surgical interventions’ but then said that no further attention is paid by Mühlhoff to such other possibilities other than the reference in [0160] to using the treatment laser to remove the epithelium, which he took to be a reference to PRK. In that way, Mr Benjamin also dismissed the significance of the teaching in [0015].
439. [0158]: The second principal issue arose in relation to the detector which could be used in the fifth embodiment. Professor Bouma was of the view that the detector of Fig 19 was limited to a MPF imaging device. He seemed to have a number of reasons for this.
440. First, because he read the final sentence of [0158] as referring to the measurement regimes shown in Figs 20-22. The consequence was that, in his view, the fifth embodiment was entirely separate to the first to fourth embodiments. Second, because Fig 19 showed the detector as a photodiode, consistent with MPF, but inconsistent with using OCT because an OCT device would not normally be described as a detector, but also because an OCT device would have several elements not shown in Fig 19. Third, because MPF would generate ‘tissue-specific signals’ which were characteristic of each tissue type, but OCT does not produce laser-induced tissue-specific signals.
441. Mr Benjamin also saw the fifth embodiment as a departure from the approach of the first to fourth embodiments, due to the use of ‘tissue-specific signals’ to produce a coordinate map of the cornea in advance of laser treatment to assist with the planning of that treatment. He was of the view that the use of MPF to achieve this tissue-specific map-building, was not a technique familiar to the SO at the Priority Date. Thus it appears Mr Benjamin adopted Professor Bouma’s views on the fifth embodiment.
442. I start with the first sentence of [0158]. In context, it is clear that the reference to the operating method mentioned at the outset is to the laser-surgical refractive error correction, first mentioned in [0005] and the subject of [0083]-[0086], which is then used as the basis for the application of the various measurement principles described in the first to fourth embodiments. The first words of [0158] clearly refer, in my view, to all the embodiments. In the second sentence, Mühlhoff specifies the precision with which the cornea can measured (apparently in any of the embodiments), with a depth resolution of 1 µm and low lateral resolution (e.g., 100 µm) from the epithelium to the endothelium (cf Figure 2 above) ‘over the entire region, in which the surgical invention should be implemented’. Thus, Mühlhoff is making it clear that it is possible to measure the whole volume of the cornea. This second sentence teaches that, as the Skilled Team would expect, the eye is held against a contact glass by suction, but measurement of it is still necessary before the surgical intervention is implemented, as the Skilled Team would expect.
443. At this point in the paragraph, Mühlhoff signals he turns specifically to the fifth embodiment and a multiphoton fluorescence (which is explained as being sensitive to differences in the different layers and/or interfaces) being detected with a spatial resolution. We then come to the final sentence: ‘Alternatively, any of the above-described measurement principles can be used.’
444. Professor Bouma was of the view that the skilled reader would read that last sentence as referring to the measurement approaches illustrated in Figs 20, 21 and 22. These are described as measurement regimes in [0153]-[0155]. However, [0032] refers to the confocal principle, [0090] refers to an OCT device as following the principle described in the Izatt article and [0134] refers to the principle of a slit lamp. Mühlhoff was precise in his use of language. I am in no doubt that the skilled reader would understand the final sentence of [0158] as referring to the measurement principles described in each of the earlier embodiments. I am also in no doubt that Professor Bouma’s reading of that sentence was perverse.
445. Thus, in [0158] Mühlhoff is indicating a preference for MPF but equally saying that any of the previously described measurement principles can be used. This conclusion is supported by Professor Bouma’s acceptance that the phrase in the penultimate sentence of [0158] as to the key characteristic of MPF, namely ‘sensitive to differences in the different layers and/or interfaces’ and allowing a spatial resolution, was equally applicable to OCT.
446. Once again, Mr Benjamin appeared to have adopted Professor Bouma’s view on [0158]. Mr Benjamin simply said he did not ‘read Mühlhoff as suggesting that any of the detection methods used in the first four embodiments can be used to generate the tissue-specific signals required for the fifth embodiment’ but without giving any reasons. Mr Benjamin understood the significance of separating the fifth embodiment from the first four because in his second report he pointed out that it is only in the fifth embodiment that imaging prior to treatment is disclosed.
447. In my view, the approach taken by Professor Bouma and Mr Benjamin to [0015] and [0158] of Mühlhoff was revealing. Instead of reading the document fairly, they were each prepared to adopt Professor Bouma’s perverse reading. This allowed them to take a highly restricted view of the disclosure of Mühlhoff. I am in no doubt that Professor Bouma understood the significance of what Mühlhoff was teaching the Skilled Team in both [0015] and [0158] and he adopted the perverse reading in order to avoid that significance. Thus, in fact, his evidence recognised (a) the force of the teaching in each of those paragraphs, and (b) that that teaching was not helpful to AMO’s case, which is why he sought to avoid it. In my view, his evidence in those regards was not the evidence of an independent expert.
448. With the understanding that Mühlhoff in fact explicitly taught that OCT, confocal microscopy and the slit lamp principle could also be used in the fifth embodiment, the remaining points relied on by Professor Bouma are easily resolved.
449. TSS: Professor Bouma (supported by Mr Benjamin) and in turn AMO in my view put far too much emphasis on the notion of tissue-specific signals when at most in Mühlhoff they are a means to the end of locating the boundaries between different layers of tissue. As Alcon put it, it is important to view the disclosure at the correct level of abstraction. In context, it seems clear that Mr Benjamin understood ‘tissue-specific signals’ as a requirement and in contradistinction to the indirect detection of specific tissues by the detection of changes in tissue at boundaries, which he appeared to ignore. Where the evidence came out was that MPF would generate TSS, but the other measurement techniques would not. However, the fact that they were not capable of producing TSS would in no way deter the Skilled Team from investigating using OCT in the fifth embodiment for example. This resolves the second sub-issue identified in paragraph 434 above.
450. Single Light Source: The issue was whether the fifth embodiment can only be implemented using a single light source. Although Professor Bouma said of using a single light source and a single set of optics (which avoided the tolerance chain issue) ‘that is the thing that is really cool about embodiment 5’, but it needs to be kept in mind that he was hunting around for other reasons to support his thesis that the fifth embodiment was limited to MPF and was incompatible with OCT. Whilst the use of a single light source is clearly a preference in Mühlhoff because it eliminates the tolerance chain, there is certainly no teaching that the tolerance chain is an insurmountable obstacle. Quite the contrary.
451. Compatibility with OCT: Professor Bouma expressed the view that the fifth embodiment was not compatible with OCT. This was for two reasons: the first was that OCT did not produce TSS; for the second, he took Figure 19 rather literally. His point was that if OCT was used in the fifth embodiment, other elements (a reference arm in particular) would need to be added. This is a point of no consequence as soon as one understands that Mühlhoff explicitly teaches using OCT in the fifth embodiment and recalls that the Skilled Team knows how to implement OCT.
452. Criticisms of Professor Mrochen: AMO levelled significant criticisms at Professor Mrochen’s evidence in relation to the fifth embodiment and OCT. In the AMO view of the fifth embodiment, these criticisms carry weight but they have less significance in view of my findings already. I deal with the points in turn:
i) The first criticism concerns the box labelled 3 in Figure 19. In his first report, Professor Mrochen had set out Fig 2 of Mühlhoff which shows a schematic of an OCT device which is labelled 3. A few pages later he turned to Fig 19 and [0149] and [0150]. From the text, he picked up that the detector was 78 and said ‘[not expressly labelled in Figure 19, which instead includes a specific embodiment of the detector, in the form of OCT device 3]’. Professor Mrochen made no reference in this report to MPF, but in response to Bouma 1, he addressed it in his second report but adhered to his point that Figure 19 showed OCT device 3, probably because Bouma 1 made no comment about the labelling 3 in Fig 19. What Professor Mrochen had overlooked were some features in or relating to Fig 19 which were inconsistent with OCT. The first was the content of the box marked 3 - it features the symbol of a photodiode; the second was a wave emanating from the tissue to the box; the third was the absence of a reference arm in Figure 19; and the fourth was the actual description in [0150]. All these features tend to confirm that Fig 19 is reflecting the use of MPF as taught in [0158]. The combination of these features is inconsistent with an OCT device. The point on the absence of a reference arm is not clear cut however. Although AMO emphasise that the light path is important for an OCT device, and it would not be normal to indicate an OCT device as in Figure 19, this is tempered by the description in [0150] where it says the ‘signal is received by detector 78 via the detection beam path (not illustrated in any more detail).’.
ii) The cross-examination on this point got mixed up with the issue over the reference in the final sentence of [0158] to ‘measurement principles’. Professor Mrochen clearly had in mind that this sentence referred back to OCT and the other measurement principles in the first to fourth embodiments. He found it difficult to separate that indication from what was signified in Fig 19. AMO criticise him for saying that Mühlhoff described OCT as a measurement principle, and for adhering to that point. As I have found, in effect, Mühlhoff does, so he cannot be criticised for adhering to that point, even if he found it difficult to separate these points.
iii) The second point I will describe as the z-coordinate issue, one which is intimately tied up with TSS and single light source. I have drawn attention to Professor Bouma’s point about the advantages of the combination of MPF, single light source, single set of optics, no tolerance chain in paragraph 450 above. His evidence was that these advantages could not be obtained if one used OCT in a fifth embodiment arrangement. If one used a single light source and set of optics for an OCT measurement beam as for the treatment laser, it would be possible to obtain a single x, y coordinate system. That would not be possible for the z coordinate, because in OCT that is determined by the position of the mirror in the reference arm and not by the focal point of the laser beam. Professor Bouma explained this as follows in his third report:
‘OCT would not generally provide signals in the same coordinate system as the treatment laser for all three dimensions (X, Y and Z) even if the same light source is used. In OCT the depth measurement is fundamentally an interferometric measurement. The measurement of signals from different depths is made by sweeping the mirror in the reference arm (in the case of time-domain OCT) or by processing the optical spectrum reflected from the entire axial length through the tissue (in the case of Fourier domain OCT). This measurement is not related to the axial position of a focal point within the sample. Even if the same deflection device was used in the measurement and treatment phases (so that there was correlation in the X-Y plane), there would be no correlation between the depth measurement provided by the OCT and the depth of treatment laser focusing in the tissue.’
iv) Professor Mrochen responded in his third report. He agreed that the z-coordinate in OCT is determined, at least in part, by interferometric measurement, but he did not agree that this meant that OCT could not be used in the fifth embodiment. He went on to say that whilst in OCT the z-co-ordinate is derived from the position of the reference mirror (in time domain OCT) or processing of the optical spectrum (in Fourier domain) and not solely the position of the focussing lens (which determines the axial position of the focal point of the laser within the sample), that does not mean that they use a different coordinate system that would need to be spatially registered. He said the SE would be able to set up the system such that the z-coordinate, derived (at least in part) by interferometric measurement during the OCT measurement step, was used to position the focussing lens to ensure the laser was targeted to the correct z depth during the treatment step.
v) Professor Mrochen also responded by referring to the teaching in Mühlhoff at [0098] and [0099] as disclosing that the axial resolution of an OCT device may be improved by using a high numerical aperture and sweeping the focal point of the OCT measurement beam through different axial depths of tissue. He said in this technique, there is a relation between the focal point of the OCT measurement beam and the z-coordinate of the measured signal.
vi) In the course of cross-examination, Counsel put to Professor Mrochen ‘Professor Bouma tells me that the Z co-ordinate OCT is determined entirely by interferometric measurement. Do you agree?’ Where this point ended up was encapsulated in the following exchanges in which Professor Mrochen confirmed what I summarised in the preceding paragraph:
20 Q. I understand that, but the point is that in any z coordinate
21 you measure, even in that OCM system, it comes from the
22 position of the reference mirror and not from the position of
23 the focal point of the beam?
24 A. Well, I would say it comes from both. I need to know where is
25 this focal point and I am scanning around.
2 Q. Within the depth of field given you by the focusing of your
3 laser, within that depth of field the z coordinate comes from
4 the position of the reference mirror; correct?
5 A. Well, yes, yes. I can see that.
vii) In my view, both experts are correct. Professor Bouma took a more theoretical approach whereas Professor Mrochen had the more practical approach reflected in his written evidence. The aim of the cross-examiner was to attempt to confine Professor Mrochen’s point to being a simple ‘depth of field’ issue, but that does not disprove what I have summarised from his evidence at paragraph v) above.
viii) The fifth point concerns X1. At the end of a long cross-examination, Professor Mrochen was handed a copy of Fig.19 and asked to draw how OCT would be realised in that arrangement. Professor Mrochen quickly drew in what appears to be a reference arm, utilising a separate light path. As was clearly intended, he did this there and then and under pressure. I do not think this was a particularly fair approach.
ix) As AMO pointed out, Alcon did not put X1 to Professor Bouma (but Alcon say they did not need to). At the conclusion of his evidence, Professor Bouma indicated he wanted to comment on a piece of evidence, which turned out to be X1. I heard his additional evidence de bene esse. He explained why what Professor Mrochen had drawn could not work. In fact, he concluded that Figure 19 could not be modified in a simple way to achieve OCT, evidence which confirms the unfairness of the X1 exercise because that, in my view, was the premise on which Fig 19 was put.
x) All of this fuss about X1 misses the point. It is yet another argument which is aimed at the wrong level of abstraction. Mühlhoff teaches that all the measurement techniques can be used in the fifth embodiment and there was no suggestion (once the issues over TSS and single light source are resolved) that OCT could not be used in a fifth embodiment type arrangement.
453. In terms of what Mühlhoff actually teaches for his fifth embodiment, Professor Mrochen turns out to be correct: OCT can be used - that is what Mühlhoff said. However, the significance of Professor Mrochen’s evidence as to the box marked 3 in Fig 19 cannot be brushed aside. As AMO submitted, it is indicative of his whole approach to Mühlhoff. It indicates Professor Mrochen went looking for OCT in Mühlhoff, and indicative of his reasoning being infected with hindsight. Furthermore, in his cross-examination, Professor Mrochen clearly lost some objectivity. I will keep this in mind when I come to consider the obviousness arguments.
454. As to the sixth point, AMO’s contention that pre-planning was only disclosed in the fifth embodiment created, at least in my mind, a conundrum as to what was envisaged in embodiments 1-4. It is all very well having the feedback loop which identifies the location of a plasma bubble as soon as the laser pulse is fired, but it does not seem possible or sensible to start firing the laser without knowing where it should be aimed. In fact, this conundrum does not arise at all because in the general teaching about the example treatment, [0086] explicitly teaches that ‘The incision of the laser-surgical instrument 1 is implemented in accordance with parameters ascertained in advance …’, teaching which was ignored by AMO’s experts. In my view, the Skilled Team would conclude that amongst the parameters ascertained in advance were the locations of where to start the laser cutting, where it continues and where it ends - in short the entire cutting pattern to excise the lenslet.
455. Having read, considered and understood the whole of Mühlhoff, the Skilled Team would appreciate, in my view, that there were two ways in which these parameters could be ascertained in advance. The first and simplest method would be to take measurements of the cornea at appropriate points to ascertain the position and size of the lenslet in the cornea, using what I might call a traditional approach (e.g. ultrasound). However, the second method which would, in my view, occur to the Skilled Team was to use the imaging system to image in advance precisely because that is explicitly taught in the fifth embodiment.
456. Leaving aside the precise measurement method(s), this, in any event, is just common sense to the Skilled Team: you cannot start firing a photodisruptive laser into eye tissue without planning where you are going to cut.
457. In my view, the Skilled Team would not perceive any sharp distinction between embodiments 1-4 and embodiment 5 in the way suggested by AMO. Instead, the Skilled Team would understand that Mühlhoff presented a range of options. In embodiments 1-4, Mühlhoff taught methods of direct feedback control of a femtosecond photodisruptive laser firing pulses into the stroma, where the cutting pattern had been ascertained from measurements made in advance, and different imaging systems tracked the laser pulses and provided the feedback to the control system. In the fifth embodiment, Mühlhoff taught a further development of that feedback/control approach where the stroma was imaged in advance, by reference to which the cutting pattern would be designed, and then the imaging system would then monitor the laser pulses to ensure they occurred in the correct pattern. Mühlhoff’s preference in the fifth embodiment was to use MPF, but then said that any of the previous measurement principles could be used. So in the fifth embodiment, Mühlhoff taught the more sophisticated (one might say, more integrated) system which involved using the imaging system to image in advance which could be used with any of the measurement techniques. Whilst the Skilled Team would understand MPF at a basic level, it was not a technique with which they were familiar or had ever used. For that reason, whilst they might be interested to investigate MPF, they would do so alongside a more familiar imaging technique, likely to be OCT.
458. Thus, what Mühlhoff disclosed to the Skilled Team was a method and apparatus for excising a lenslet from the cornea of the eye in order to correct a refractive error, using a state of the art laser (in the femtosecond range) to make the appropriate incision which is guided and controlled by an imaging system which is used to image the tissue to be treated and then to control the laser. The Skilled Team would recognise the degree of precision promised in Mühlhoff - imaging down to 1µm or lower. They would also recognise that in one sense, Mühlhoff left the choice of the imaging system to them.
459. Both the SE and the SO would have particular interest in the teaching in [0015] as to applications which Mühlhoff says his invention (essentially of the combination of the precision-guided ultrashort pulsed laser) is particularly suitable, noting the promise that collateral tissue damage is largely precluded. [0015] is significant precisely because it is Mühlhoff telling the Skilled Team that his invention is applicable for many other applications, with particular emphasis on other ophthalmological interventions, and even more particularly for incisions in the lens. In terms of what that phrase (incisions in the lens) would trigger in the mind of the Skilled Team, it seems there are at most four possibilities: an incision for AC, an incision for PCO, lens fragmentation and possibly incisions in the nucleus to soften the lens. Far from this being hyperbole, the suggestion would appear to the Skilled Team to be entirely sensible and serious.
460. In the light of this teaching, the Skilled Team would understand that Mühlhoff presents a range of options as to what ‘the invention’ (as referred to in [0015]) is. One point which came out very clearly from the evidence is that the Skilled Team would adapt the teaching to the particular application they were considering.
461. Applying the Pozzoli approach, I have identified the Skilled Team and summarised their CGK above.
462. For reasons which will become apparent, I remind myself here of my findings as to CGK on two key topics: femtosecond lasers and OCT imaging:
i) Femtosecond lasers were proven for femto-LASIK. The Skilled Team had an expectation that femtosecond lasers would prove capable of being used to make incisions inside the eye without causing undue collateral damage.
ii) The Skilled Team (via the SE) had an expectation that OCT was able to image the anterior segment of the eye so as to identify the location of the lens capsule, the lens and the lens nucleus.
463. There is, of course, a difference between those findings and the basis on which Professors Mrochen and Lawless put forward their views on obviousness. To repeat, they proceeded on the basis that the following was CGK:
i) Knowledge of the successful use of OCT to take measurements across the whole eye; and
ii) Knowledge of the successful use of femtosecond lasers in making precise and accurate incisions in the cornea (in the context of flap creation in LASIK) and other structures in the eye such as the lens.
464. The differences are subtle. In each case, the difference is between knowledge of successful use versus an expectation that such use would be successful.
465. I have also identified the inventive concept of claim 1 of each of EP861 and EP528, and the additional point in their claims 2 and 6 respectively. As for the third step, the differences between Mühlhoff and claim 1 of EP861 and EP528, respectively, are that Mühlhoff does not disclose using its apparatus for AC or LF. AMO submitted there was a further difference: that Mühlhoff does not disclose pre-planning as required by each claim 1. Whether this is a difference or not depends on the starting point and I consider this below.
466. So far as claim 2 of EP861 and claim 6 of EP528 are concerned, the additional difference is that Mühlhoff does not disclose bottom-up scanning.
467. In approaching the fourth step, I remind myself of course, that the Patents must be left entirely out of account.
468. In closing, Alcon put forward two arguments. Both arguments, as I understand it, start from [0015] which put the Skilled Team in mind of investigating Mühlhoff’s teaching using a pulsed femtosecond laser for, amongst other things, performing an AC and, separately, LF. The validity and force of this starting point were reinforced by the frankly bizarre attempts by AMO’s witnesses to deflect, defuse or ignore it, discussed above.
469. So far as the apparatus and method are concerned, proceeding from [0015], Alcon’s primary argument was founded on the first embodiment. In that embodiment Mühlhoff does not describe imaging in advance with OCT to guide where to make the laser incision, even though it is taught in the fifth embodiment.
470. Even though there is no OCT imaging in advance, Mühlhoff still makes clear that some measurements had to have been made in advance in order to decide where the start cutting - see [0086] ‘The incision of the laser-surgical instrument is implemented in accordance with parameters ascertained in advance ….’ Although these parameters include the position and size of the partial volume of the stroma which is to be removed, those parameters mean that the stroma must have been measured in advance. As both Professors Mrochen and Lawless pointed out in their written evidence, for this type of corneal procedure, the eye of the patient would be secured with a contact glass which serves as a reference point from which the laser could be focused appropriately so as to start the incision at an appropriate point. Counsel for AMO challenged Professor Lawless on the basis that Mühlhoff’s first four embodiments did not disclose eye docking, but the Professor said the docking appeared to be necessary to produce what Mühlhoff was describing i.e. the excision of the corneal lenslet. I agree - a contact glass was completely standard for this type of corneal procedure.
471. However, for the applications now under consideration by the Skilled Team they would immediately appreciate that the contact glass is not a reliable reference point because the lens is far deeper in the eye, there is patient-to-patient variation and it may well be necessary to account for tilting of the eye even against a contact glass.
472. To make any incision in the lens using a laser, the Skilled Team would immediately appreciate the need to start the incision in the correct place and that the OCT system as configured in the first embodiment would not enable that to happen. If (as I have held) it was CGK that OCT was able to image the lens with sufficient accuracy to locate the lens capsule (and the lens nucleus), the Skilled Team would also immediately appreciate that they needed to use the OCT system (and they would have in mind a Fourier-domain system) to image the eye in advance to plan where to direct the laser pulses.
473. It is on this basis that Alcon submit that the claims 1 of EP861 and EP528 were both obvious.
474. AMO put forward a raft of points as to why no such conclusion was correct. I will deal with those which appeared to me to have some significance:
i) First, AMO relied on some evidence from Mr Benjamin that the reference in [0015] to ‘incisions … in the lens’ does not imply either AC or LF because he said neither of those involved ‘incisions’, which he said implied a knife or scalpel. He said that an AC involves a ‘tearing’ and LF involves ‘sculpting’. In the context of Mühlhoff, these answers made no sense. When I asked him what the phrase would conjure up in the mind of the SO, he said ‘the laser does not really incise’ and then he fell back on lens softening. His answers were those of an expert avoiding the obvious. His continued resistance on this issue did him no credit, in my view.
ii) Second, AMO relied on Professor Bouma’s evidence that [0015] contained hyperbolic statements by Mühlhoff, a point I have dismissed already.
iii) Third, AMO submitted that before the Skilled Team would start considering whether it might be worth trying to apply Mühlhoff’s teaching to applications outside the cornea, they would first want to know whether Mühlhoff would work as described. Although Professor Mrochen agreed with this proposition, I observe it is circular and self-defeating. If this proposition was correct, before implementing Mühlhoff for incising a lenslet from the cornea, the Skilled Team would want to see that apparatus working as described. That, in my view, would not be the reaction of the Skilled Team who had read Mühlhoff with interest.
iv) Fourth (and relatedly), AMO submitted that Mühlhoff had not been shown to work and was a mere paper proposal. They sought to bolster that submission by pointing to a number of technical obstacles to implementation that they said Professor Mrochen agreed with in his cross-examination. Overall, however, Professor Mrochen was clear that the Skilled Team would be able to overcome the series of technical challenges involved in creating the system taught. If they were not, then the same position would apply to both Patents and they would both be insufficient. I can leave this point on one side.
v) Fifth, AMO pointed to evidence from Mr Benjamin to the effect that his SO would have a major concern as to the smoothness of the incision in the anterior capsulotomy. In this answer, he seemed to be conjuring up an image of the prior ‘can-opener’ type capsulotomy. Even if the SO had this concern, the SE would put him straight immediately. A properly programmed femtosecond laser would be able to make an incision in the anterior capsule that was far smoother than those achieved in the ‘can-opener’ technique. I do not consider this would have been a concern at all, let alone a major concern. It would certainly not have put the Skilled Team off investigating.
vi) Sixth, AMO submitted that in the first embodiment, Mühlhoff does not disclose acquiring an OCT image or using it to determine parameters for a cutting pattern which is then executed by the laser and delivery system. This is true, but Alcon’s argument does not assume otherwise. AMO further submitted that any suggestion that to do so was obvious is pure hindsight. This suggestion was in part founded on AMO’s view of Mühlhoff which I have found to be wrong. On the disclosure of Mühlhoff I have found, I do not consider this step does involves hindsight. Even though this argument proceeds from the first embodiment, Mühlhoff expressly teaches pre-planning in advance in the fifth embodiment - which, of course, the Skilled Team has considered.
vii) Seventh, AMO observed that the suggestion being made by Alcon in this part of the case was that because Mühlhoff says, in his first embodiment, that OCT can determine the position of a plasma bubble relative to the epithelium and/or endothelium of the cornea, OCT would also be understood to be capable of and suitable for determining the absolute location of the anterior capsule so as to enable the laser to be targeted to that location. This is indeed the suggestion in Alcon’s argument. However, AMO submitted that did not follow at all and the suggestion that it did was, once again, pure hindsight. Once again, I disagree. Again, if it was the case that the Skilled Team were not able from their CGK to build an OCT system which was capable of and suitable for determining the absolute location of the anterior capsule, both Patents would be insufficient. It does not require hindsight for the Skilled Team to think about using the OCT imaging system which is already controlling the laser to create an image in advance in circumstances where the laser is not going to be fired without the Skilled Team knowing where the photodisruptive pulses will have their effect.
viii) Eighth, AMO sought to examine a project in which Professor Mrochen was involved at and after the Priority Date when consulting for Wavelight. The suggestion was that Professor Mrochen had read Mühlhoff but did not spot what is now contended to be obvious. His evidence did not support this suggestion. Professor Mrochen stated he was not involved in the development of the femtosecond laser for cataract surgery at Wavelight. Although there was some development work, his understanding was it was not implemented at least in part due to patent concerns.
ix) Ninth, AMO make effectively the same hindsight point as for Freedman, to the effect that both Professors had exaggerated the state of CGK as regards both femtosecond lasers and OCT imaging. However, this exaggeration is eliminated, since I proceed on the basis of my findings as to these two key points of CGK.
x) Tenth and finally, AMO submitted that Professors Mrochen and Lawless were infected with hindsight knowledge of (a) the success of the SMILE procedure i.e. the use of a femtosecond laser to excise the lenslet, as taught in Mühlhoff and (b) the Patents and the modern systems from each of the parties which reflect their teaching.
475. Standing back from the detailed points, but with their content in mind, there are two points to consider. The first is hindsight (including in particular AMO’s tenth point) and the second is the overall question as to whether the principal claims of each of EP861 and EP528 were obvious.
476. I first consider whether this obviousness case is itself tainted by the hindsight which tainted some of the views expressed by Professors Lawless and Mrochen. Most of those related either to the CGK position or to aspects of the disclosure of Mühlhoff, all of which I have corrected. I do not consider there is any residual hindsight which infects the obviousness analysis. On the CGK issue, the effect of the subtle difference between my findings and the basis on which the Professors proceeded would have simply increased the motivation of the Skilled Team to try such a system, but on the basis of my findings as to the CGK, the Skilled Team would already have had more than sufficient motivation to investigate such a system.
477. Applying my CGK findings summarised at paragraph 462 above, I adopt the reasoning in paragraphs 468 to 473 above, which neither involves nor requires any hindsight. I conclude that claims 1 of both EP861 and EP528 were obvious over the first embodiment of Mühlhoff. In summary:
i) In the first embodiment the link between the femtosecond disruptive laser and control by the OCT system is explicit.
ii) The prompt to consider use to make ‘incisions in the lens’ is explicit.
iii) The step to use the OCT system to image in advance so that the laser incision occurs in the right place is modest.
478. This reasoning provides the Skilled Team with systems which land in claim 1 of EP861 and in claim 1 of EP528. I also point out that both Patents are ‘ideas’ patents. By the point reached in paragraph 472 above, the Skilled Team have reached the idea in claim 1 of each Patent. Based on my findings as to the key CGK, these ideas would have been well worth investigating for the Skilled Team.
479. The critical point is that, in his first embodiment, Mühlhoff contains convincing teaching of the use of a pulsed femtosecond laser used in the stroma to make precise and accurate incisions, measured and controlled using an OCT system i.e. Mühlhoff taught the combination of the laser controlled by the OCT system. When considering applying that teaching to the suggestion of using it to make incisions in the lens, it was, in my view, immediately obvious to the Skilled Team that they would have to image in advance so they knew where to place the laser pulses and that they should use the imaging system they had already to do so.
480. Let me assume however, that those claims were not obvious over the first embodiment of Mühlhoff. In my view, that could only be for some reason based on AMO’s contentions as to the CGK. But based on those contentions or if the key CGK was deficient in some other material way, both Patents would be insufficient.
481. Alcon’s secondary argument on Mühlhoff was put forward on the basis that, contrary to their primary position, the fifth embodiment was expressly disclosed as limited to one in which only multiphoton fluorescence imaging was used. In that case, Alcon argued that it was obvious to modify the fifth embodiment to use OCT imaging instead.
482. Since I have found that Mühlhoff expressly teaches using OCT in the fifth embodiment (at the end of [0158]), I will consider this secondary argument on that basis.
483. Although Mühlhoff expresses his preference in the fifth embodiment for the use of MPF, the Skilled Team is not particularly familiar with that technique. Whilst they may investigate MPF, they would do so alongside OCT, with their knowledge of recent developments and the capabilities of Fourier-domain OCT.
484. This then raises AMO’s case and Professor Bouma’s evidence that:
i) The fifth embodiment was limited to tissue-specific signals, which OCT could not detect;
ii) The apparatus depicted in Fig 19 (i.e. with a single laser source for both imaging and treatment) could not be made to work using OCT (which includes the X1 issue).
485. Both these points were, as Alcon put it, the tail wagging the dog. For the Skilled Team following Mühlhoff’s suggestion that any of the imaging principles described earlier (including OCT) could be used in the fifth embodiment, they would naturally understand they would have to make suitable alterations to what Fig 19 depicted and they would not be restricted to attempting to implement precisely that set-up (which seems to me to be what Professor Bouma had in mind, bearing in mind his evidence that the SE was limited to implementing a specification presented to him or her). Furthermore, the Skilled Team would not get hung up on ‘tissue-specific signals’ since they would know that OCT was capable of detecting the boundaries between different types of tissue and that was what was required to ensure the laser was cutting in the right place.
486. The fifth embodiment explicitly discloses imaging in advance of treatment to plan and guide the treatment laser.
487. With the same starting point in [0015], and based on the Skilled Team choosing to use OCT, I am entirely satisfied that it was obvious to proceed from the fifth embodiment using OCT to perform AC and LF.
488. I mention that Alcon were prepared to put their obviousness arguments on alternative bases: either that the previous attempts to use lasers to perform AC and LF were part of the CGK or not. I have not found it necessary to rely on one alternative or the other. With such knowledge, the motivation to proceed with the femtosecond laser teaching in Mühlhoff would be somewhat stronger, but even without such knowledge, the Skilled Team would have sufficient motivation to proceed.
Claim 2 of EP861 and claim 6 of EP528
489. Both claims add the additional integer which can conveniently be summarised as the use of ‘scanning up’ laser incision. Professor Bouma expressed the view that this feature constituted real insight on the part of the inventors.
490. I have found above that this placing of laser pulses was CGK, and on that basis these claims were obvious. Anyone with practical experience of experimenting with laser pulses in ophthalmic tissue would have experienced the problem to which scanning up was the solution and I have already found the Skilled Team had such practical experience. A principal reason why Professor Bouma expressed his view was because he had no such experience.
491. Let me assume however that I am wrong that this technique was CGK. Alcon submitted that there were two possibilities from which the Skilled Team could chose: scanning up or scanning down, either being obvious. If the Skilled Team started with scanning down, they would quickly find the interference effect of gas bubbles in the tissue and switch to scanning up.
492. AMO’s answer to all this was first, scanning up was not CGK; second, all this was based on hindsight because Professor Mrochen had gone looking for mentions of this technique in various textbooks and third, it cannot have been obvious because the Vogel group did not mention this when reporting their experience of the problem whilst conducting their experiments on using picosecond lasers for intrastromal refractive surgery.
493. On the third point, I accept that the Vogel paper does not mention this solution but that paper was more than 10 years before the priority date. Vogel does discuss the problem of bubbles from earlier pulses interfering with later laser pulses, but in a different context in which scanning up was not the solution. This is the reason, I find, as to why Vogel does not mention scanning up.
494. In the part of the paper put to Professor Mrochen Vogel’s group was investigating the use of picosecond lasers for intrastromal evaporation of a layer in the stroma in order to effect a refractive adjustment. Figure 8 indicates that laser pulses of 80mJ in (a) and 300µJ in (b) were applied from the right-hand side as the corneal specimens were moved in a vertical direction. Fig 8(a) indicates that the single large cavity produced was between 0.1-0.2mm deep and 2-2.5mm in length, less than 10 seconds after laser exposure, the cavity disappearing completely after approximately 1 hour. Fig 8(b) shows multiple cavities of uneven size, roughly making up a shape of equivalent dimensions. The problem discussed was that the volume of evaporated tissue is small compared to the tissue displacement caused by the expansion of the laser plasma. It is the large cavities which disturb the optical properties of the cornea. The bubbles from earlier pulses reflect and refract the light of the subsequent laser pulses. The overall effect was that ‘it is not always possible to evaporate a homogenous layer of definite thickness’, which is what an intrastromal technique requires. There is no mention of scanning depth wise in the tissue at all (i.e. left to right or vice versa in Fig 8), only horizontally (i.e. vertically in Fig 8). As I said, Vogel does not suggest the scanning up solution because that was not the solution to the problem they experienced in their context.
495. On the second point, in my view there was no hindsight in Professor Mrochen’s approach. He expressed the view that this additional feature of scanning up was obvious. He gave a range of reasons in support, reasons which I find convincing. To summarise, he said that the Skilled Team would be conscious of the importance of accurate control over the focal point of the laser and aware of the potential for gas bubbles from previous pulses to interfere with the optical path and the positioning of the focal point of the laser for subsequent pulses. The Skilled Team would also be aware that these gas bubbles remain present in the tissue for significantly longer (he estimated several whole seconds for femtosecond pulses) than the time it would take to perform the next scan (less than a second). He was entitled to point to mentions in textbooks of this problem being experienced and this scanning up solution in order to support his reasoning.
496. Having identified this having been mentioned in two textbooks, it is perhaps not surprising that in his second report, he suggested that the phenomenon and the solution to it were very well known by the SE by the priority date, notwithstanding the fact that he had not explicitly identified this as CGK in his first report. Bearing in mind AMO’s whole approach, they attacked him for again searching around for these textbooks. As I have already indicated, it was a natural reaction for Professor Mrochen to look for and to mention materials which supports his view when it was challenged. ‘Hindsight’ is an easy accusation to throw around in these cases, but the accusation is an empty one if the reasons in favour of obviousness are convincing.
497. I am entirely satisfied that this feature of scanning up was obvious not least because, even if they were not previously aware of this technique, when the Skilled Team started experimenting with their OCT-guided femtosecond laser system to make incisions in bovine or porcine lens, they were bound to experience the problem. The scanning up solution would have been lying in the path in front of them - ob via.
Secondary evidence
498. Certain arguments were made as to pieces of secondary evidence which support obviousness or not which I consider here.
499. Even though not a major plank of their case, AMO pose the traditional question: if either Patent was obvious, why were they not done before? However, I am satisfied that in the particular circumstances of this art, this consideration does not point away from obviousness. As Alcon submitted, the two principal components of the system (femtosecond laser and OCT for imaging and guidance) had not been available for so long before the Priority Date that it can be said that all the obvious uses of them in eye surgery must have been thought of and publicly disclosed by the priority date. Furthermore, Mühlhoff was published only 10 months before the priority date. As Professor Bouma explained, it was Fourier domain OCT which transformed the clinical use of OCT, but the first commercially available Fourier domain OCT device was not available until after the priority date in 2006. In any event, it took AMO six years to launch a commercial device implementing the Patents. Furthermore, in this art it was not automatically the case that what was technically obvious would be done, due to commercial considerations.
500. Alcon relied on certain references in textbooks which they suggested provided secondary evidence of obviousness. First, Kurtz’s chapter concludes with a short section headed ‘Other Ophthalmic Applications’:
‘Other obvious targets include the rest of the transparent ocular tissues (lens, capsule, and vitreous) as well as surgical procedures in translucent tissues such as the sclera. In the lens, potential applications under investigation include tissue cutting and removal for cataract and/or restoration of accommodation. …..’
501. Kurtz states his conclusions in an optimistic fashion which is a characteristic of this type of scientific writing:
The minimally invasive, high-precision characteristics of femtosecond laser technology make it highly promising for various ophthalmic surgical procedures. A number of initial applications in the cornea are already in clinical use and/or commercial development. Continued advances in procedures and technology will likely lead to expanded use of this technology in ophthalmology and possibly in other medical fields as well.
502. From a technical standpoint, Kurtz was correct but the issue was whether there was a sufficient commercial justification to develop further applications. Be that as it may, the former quote provides, in my view, powerful secondary evidence of obviousness.
503. Against that, AMO point to the conclusions in the Dodick Chapter in Steinert, which end with these two paragraphs:
‘The biggest limitation of the current laser systems is the challenge of denser cataracts. Given the rapidly evolving refinements and advances made in the technology to date, however, it is likely that this problem will be overcome.
What does the future hold? Perhaps, by making ultra-small incision cataract surgery a reality, laser cataract surgery has opened the door to true endocapsular surgery. Maybe the probes of the future will allow for anterior capsule puncture, and on completion of lens removal, perhaps the capsular bag will be reinflated with an injectable lens, allowing for the preservation of accommodation. One can only guess at the directions this rapidly advancing technology will take, but one thing is sure: lasers are expanding the frontier of cataract surgery.’
504. However, these concluding remarks seem to me to reflect two particular features of the authors of this chapter. The first was a heavy emphasis on phacoemulsification and lens removal. The second was that in their speculations as to ‘true endocapsular surgery’, these authors were looking many years into the future and far beyond immediate applications. So, these remarks do not point away from obviousness.
505. In the other two textbooks relied upon, it is apparent that both Niemz and Lubatschowski restricted themselves to applications which had actually been demonstrated and neither commented on other potential applications. So, these texts are neutral.
506. Overall, the secondary evidence provides some support for the obviousness of claims 1 of each Patent.
507. At various points in my assessment of the obviousness arguments on the principal claims of each Patent, I have indicated that if those claims were not obvious, they would be invalid for insufficiency. It is convenient to mention a general consideration here which I had in mind at each of those various points. I considered whether there was some middle ground between obviousness and insufficiency where the Patents would or might remain valid.
508. No such submission was made to me, no doubt because insufficiency was very largely ignored during the trial. On reviewing the expert evidence, I do not consider it would support any such submission either. When he commented on the insufficiency allegations, Professor Bouma blithely said the Skilled Team would be able to implement the feature in question without any difficulty. There was a marked contrast between those pieces of his evidence and the obstacles he constructed for the obviousness allegations - his evidence was not consistent.
509. A Schlumberger-type case would be an example where that middle ground would or might exist. This is not a Schlumberger-type case. Furthermore, I am satisfied that in the circumstances of this case, there is no such middle ground.
510. For the reasons stated above, I find both EP861 and EP528 to be invalid, primarily for obviousness but if not, because both patents would be insufficient.
511. In the usual way, this Judgment will be handed down remotely. I will adjourn further consideration to a form of order hearing on a date to be fixed and in the meantime, I will direct that time for filing any Appellant’s Notice will not run until that further hearing.

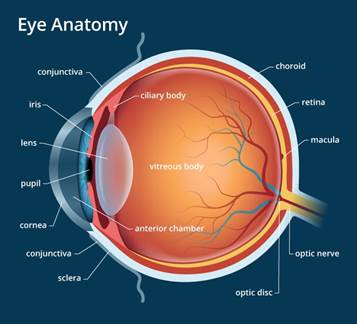
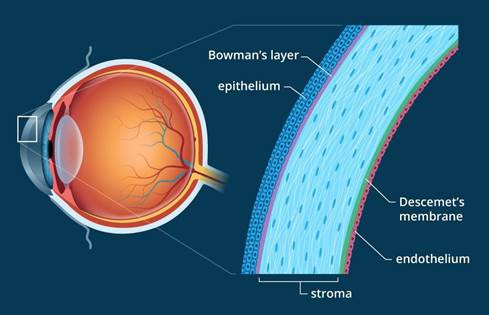
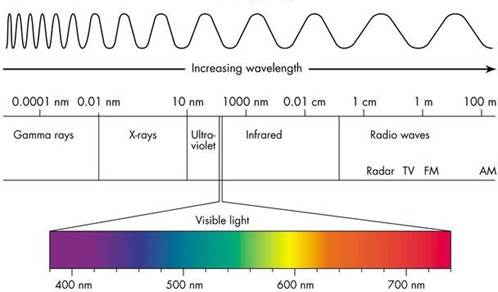
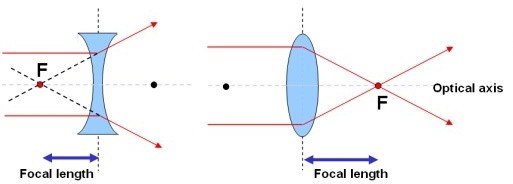
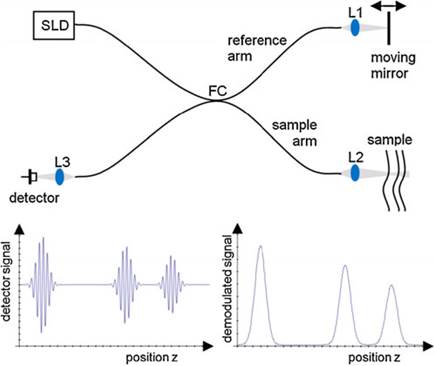
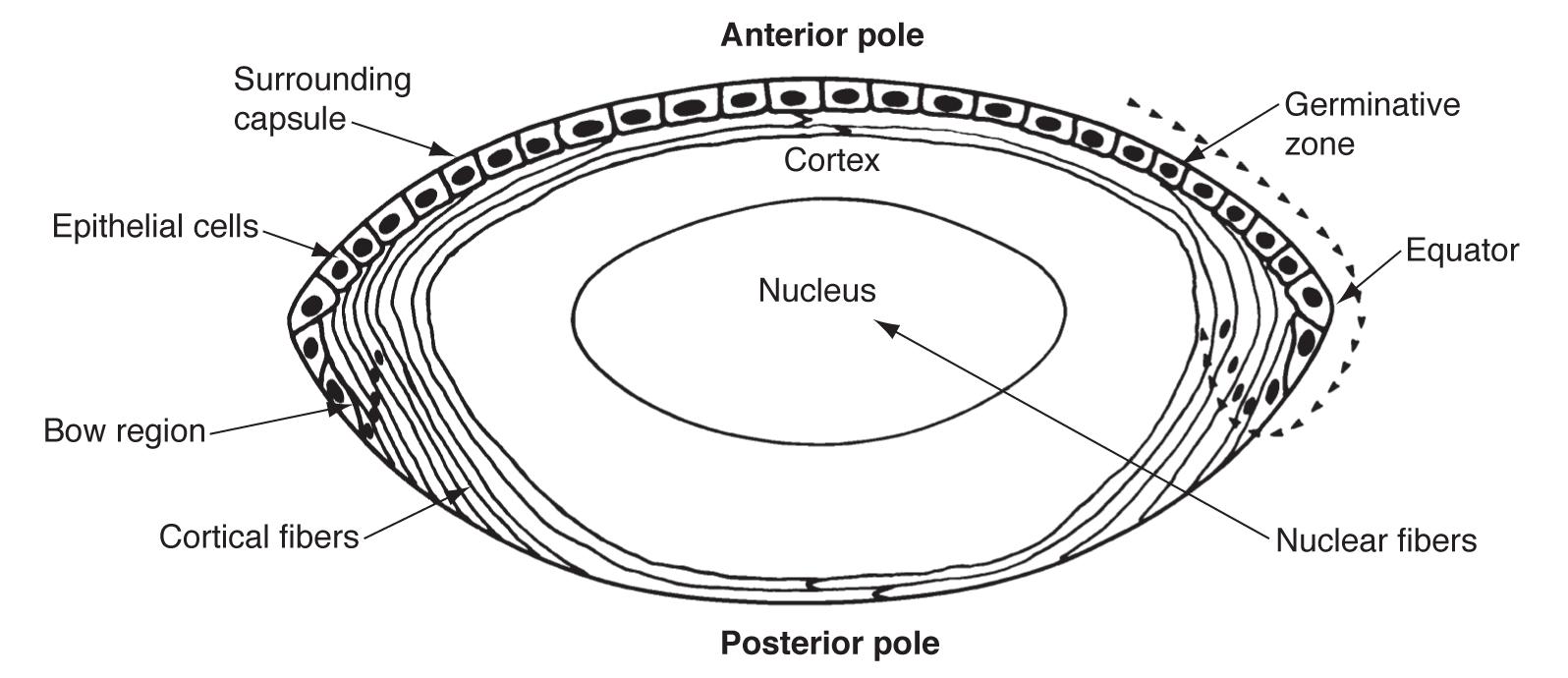{kind=link}